Few words on an ultrasound report set off more quiet worry than "thyroid nodule," especially when the scan was for something unrelated, a sore throat, a neck check, a carotid study. Here is the reassuring starting point: thyroid nodules are extremely common, the large majority are completely benign, and finding one is far more often the start of a simple watch-and-recheck plan than the start of bad news. This article explains what the radiologist actually saw, why nodules form, what those TI-RADS scores mean, and when one genuinely needs a closer look.
What does "thyroid nodule" mean?
The thyroid is a small, butterfly-shaped gland at the base of the front of your neck. It makes the hormones that set your body's metabolic pace. A thyroid nodule is simply a lump, a discrete area of tissue that looks or feels different from the rest of the gland. It can be solid, fluid-filled (a cyst), or a mix of both.
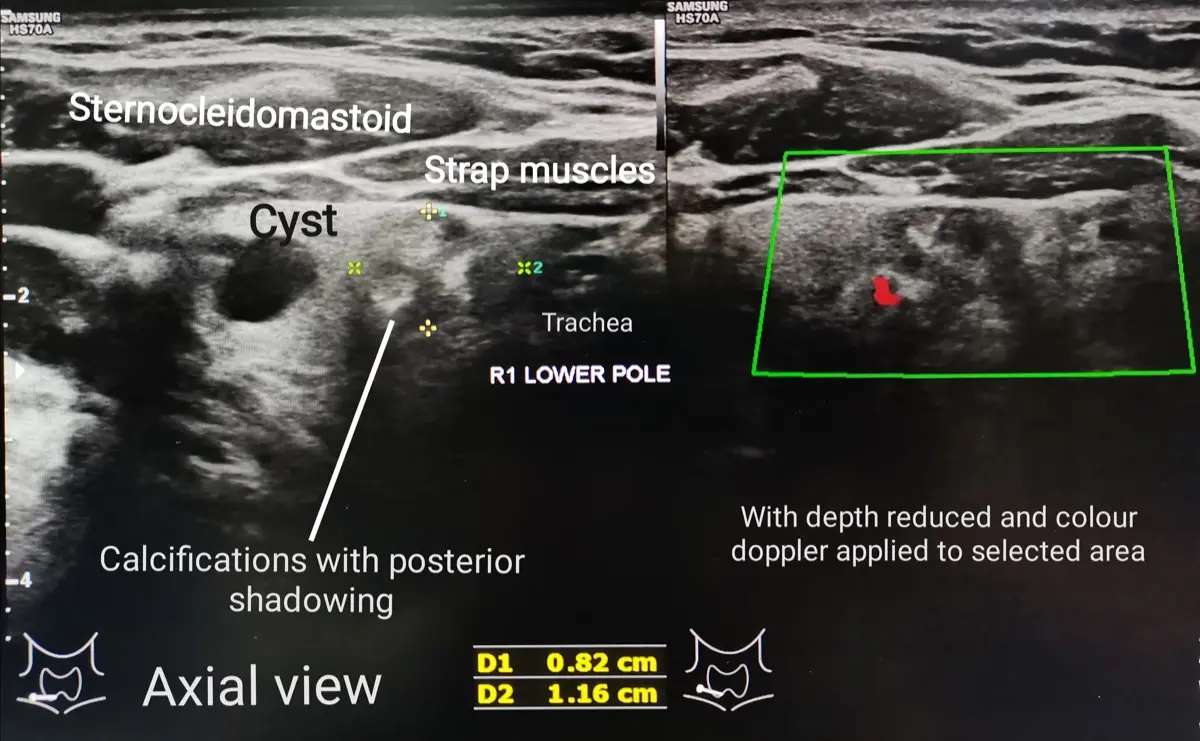
Ultrasound is the best tool for examining the thyroid because the gland sits just under the skin, perfectly placed for a sound-wave picture with no radiation. On the screen, the radiologist looks closely at the nodule's makeup: whether it is solid or fluid, its shape, how crisp or fuzzy its edges are, and whether it contains tiny bright flecks. These details matter far more than the simple fact that a nodule is there.
- Colloid nodules, the most common kind, harmless overgrowths of normal thyroid tissue.
- Cysts, fluid-filled sacs, almost always benign, similar in spirit to a renal cyst or an ovarian cyst elsewhere in the body.
- Adenomas, benign solid growths, some of which quietly make extra hormone.
Common causes and risk factors
Most nodules form for reasons no one can pinpoint, simply as part of how the thyroid changes with age. They become more common the older we get, and they are found far more often in women. Several things make them more likely, though none is a verdict:
- Getting older, nodules are very common by middle age and beyond.
- Being female, and hormonal changes such as pregnancy.
- A family history of thyroid nodules or thyroid disease.
- Iodine deficiency in the diet (less common where salt is iodized).
- Past radiation exposure to the head or neck, especially in childhood.
The single most important risk factor for the rare cancerous nodule is prior radiation to the neck. For everyone else, a nodule is usually just a normal feature of an aging gland, not a sign that anything has gone wrong.
What TI-RADS means on your report
You may see a code like "TR3" or "TI-RADS 4" on your report. TI-RADS (Thyroid Imaging Reporting and Data System) is a scoring method radiologists use to put a number on how suspicious a nodule looks, running from TR1 (benign) up to TR5 (highly suspicious). The score adds up points for features such as a solid composition, a taller-than-wide shape, irregular margins, and tiny bright specks called microcalcifications.
The score is not a diagnosis. It is a structured way of saying "this one looks reassuring" or "this one earns a closer look," and, combined with the nodule's size, it tells your doctor whether a biopsy is worth doing. The American College of Radiology TI-RADS system is the most widely used version.
Are they serious?
For most people, no. The overwhelming majority of thyroid nodules are benign, and even among the small number that turn out to be cancer, the most common type (papillary thyroid cancer) is typically slow-growing and highly treatable. A nodule found by chance on a scan done for another reason is rarely an emergency.
That said, this is a finding doctors do follow carefully, because the goal is to catch the rare problematic nodule early while leaving the many harmless ones alone. Certain features, a hard, fixed lump, rapid growth, persistent hoarseness, or swollen neck lymph nodes, prompt a more prompt evaluation. These are the exception, not the rule.
Symptoms
Most thyroid nodules cause no symptoms whatsoever, which is exactly why so many are discovered by accident. When they do make themselves known, it is usually a larger nodule felt as a lump in the front of the neck, or occasionally a vague sense of pressure, a tickle when swallowing, or a change in the voice.
A minority of nodules are "hot", they make thyroid hormone on their own. These can cause symptoms of an overactive thyroid: a fast or pounding heartbeat, unexplained weight loss, feeling warm or jittery, or trouble sleeping. A simple blood test (TSH) checks for this and helps guide what happens next.
How are thyroid nodules diagnosed and followed up?
The workup is usually quick and stepwise. Ultrasound describes the nodule and assigns a TI-RADS level. A blood test checks thyroid hormone levels. If the ultrasound features and size cross the threshold for concern, the next step is a fine-needle aspiration (FNA), a thin needle, guided by ultrasound, takes a tiny tissue sample with little more discomfort than a blood draw.
Many nodules never need a needle at all. Small or clearly benign-looking nodules are simply rechecked with a repeat ultrasound after a set interval to confirm they are stable. As with other common incidental findings such as a breast fibroadenoma, the plan depends far more on the specific features and your clinical picture than on the word "nodule" alone.
Treatment options
Treatment is matched to what the nodule turns out to be:
- Active surveillance, for benign or low-suspicion nodules, periodic ultrasound to confirm stability is usually all that is needed.
- Treating an overactive nodule, a "hot" nodule making excess hormone can be managed with medication, radioactive iodine, or, in some cases, surgery.
- Surgery, reserved for nodules that are cancerous, strongly suspicious, very large, or causing pressure symptoms.
- Newer options, for selected benign nodules, ablation techniques can shrink a bothersome lump without removing the gland.
For the typical small, benign nodule, "treatment" is often nothing more than a calendar reminder for the next scan.
Why a second read can help
Thyroid ultrasound rests heavily on judgment, two radiologists can describe the same nodule's margins, shape, or calcifications a little differently, and those subtle calls are exactly what decide whether a biopsy is recommended. If your report is borderline, gives a TI-RADS score that sits on a threshold, or simply leaves you unsure whether to watch or biopsy, an expert second read can confirm what the images really show and help you ask your doctor the right questions. DocOrbit offers a fast, independent radiology second opinion you can share directly with your physician, useful any time the next step is not obvious. You can read more about when a second radiological opinion is worth it.
Are thyroid nodules usually cancer?
No. The large majority of thyroid nodules are benign. Across all nodules found on ultrasound, only a small fraction turn out to be cancer, and those that are tend to be slow-growing and highly treatable. The point of the ultrasound and any follow-up is simply to sort the few that need a closer look from the many that do not.
What does a TI-RADS score mean?
TI-RADS is a scoring system radiologists use to estimate how suspicious a thyroid nodule looks on ultrasound, from TR1 (benign) to TR5 (highly suspicious). The score is based on features like whether the nodule is solid or fluid-filled, its shape, its margins, and whether it contains tiny bright specks. A higher score, combined with the nodule's size, guides whether a biopsy is recommended.
Do all thyroid nodules need a biopsy?
No. Most do not. A biopsy (a fine-needle aspiration) is generally reserved for nodules that reach a size threshold for their level of suspicion on ultrasound. Many small or clearly benign-looking nodules are simply watched with a repeat scan, and purely fluid-filled cysts almost never need a needle.
What are the symptoms of a thyroid nodule?
Most thyroid nodules cause no symptoms at all and are found by chance. Larger ones can occasionally be felt as a lump in the front of the neck, or rarely cause a sense of pressure, difficulty swallowing, or hoarseness. A small number of nodules make extra thyroid hormone, which can cause symptoms like a racing heart, weight loss, or feeling on edge.
Can a thyroid nodule go away on its own?
Sometimes. Nodules that are mostly fluid (cysts) can shrink or drain on their own, and small benign nodules may stay the same size for years. Solid nodules usually persist, but staying the same is reassuring. What matters more than disappearing is whether the nodule stays stable over time, which is what follow-up scans check.
Key takeaways
- Thyroid nodules are very common and the large majority are benign.
- Ultrasound describes the nodule and gives a TI-RADS score from TR1 (benign) to TR5 (suspicious).
- Most nodules need only periodic rechecks; a biopsy is reserved for those that cross a size-and-suspicion threshold.
- Even when a nodule is cancer, the common type is usually slow-growing and highly treatable.
- A hard, rapidly growing lump, persistent hoarseness, or swollen neck nodes deserves prompt evaluation.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.