Finding a lump in your breast, or seeing the word "fibroadenoma" on an ultrasound or mammogram report, is understandably nerve-wracking. Here is the reassuring truth most people are looking for first: a fibroadenoma is the most common benign breast lump, particularly in women in their twenties and thirties, and it is not cancer. This article explains what radiologists actually see, why these lumps form, when they need follow-up, and what your options are.
What does "fibroadenoma" mean?
A fibroadenoma is a solid, non-cancerous growth built from two of the breast's own normal tissues: glandular tissue (the milk-making part) and fibrous, supportive connective tissue. The name itself tells you what it is made of: "fibro" for the connective tissue and "adenoma" for the glandular part. It is essentially an overgrowth of normal building blocks, not abnormal or malignant cells.
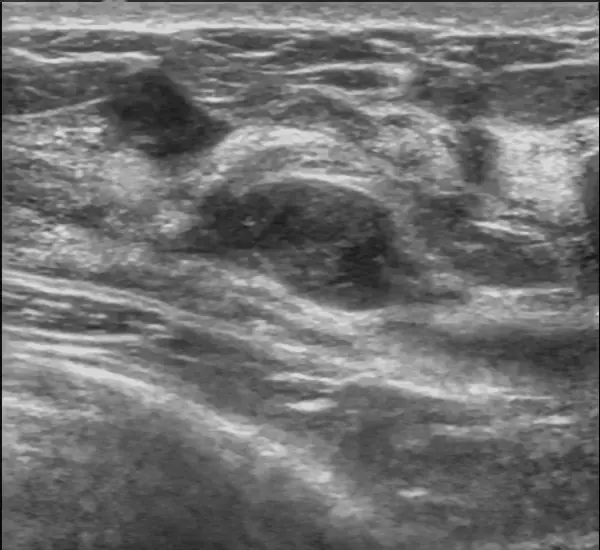
On a breast ultrasound, a classic fibroadenoma has a recognizable look. Radiologists describe it as:
- Oval and well-defined, with smooth or gently lobulated edges
- "Wider-than-tall": it lies parallel to the skin rather than standing upright
- Uniformly darker (hypoechoic) than the surrounding tissue, with no aggressive features
- Often mobile: it tends to slide under the probe rather than being fixed in place
On a mammogram it shows up as a round or oval mass with clear borders, and older, shrinking fibroadenomas can develop coarse "popcorn" calcifications that are themselves a benign sign. Radiologists usually summarize their level of concern with a standardized BI-RADS category: a textbook fibroadenoma is often labeled BI-RADS 2 (benign) or BI-RADS 3 (probably benign), the latter prompting a short-interval recheck rather than a biopsy.
Common causes
The precise trigger for a fibroadenoma is not fully known, but the strongest thread is hormonal: these lumps are sensitive to estrogen. That sensitivity explains the pattern doctors see:
- They are most common during the reproductive years, when estrogen levels are highest
- They can enlarge during pregnancy and breastfeeding, or with hormone-containing medication
- They often shrink or stop being palpable after menopause, as estrogen falls
Importantly, a fibroadenoma is not the result of anything you ate, drank, or did. Caffeine, deodorant, and minor breast trauma do not cause them. They are a normal-tissue response to the body's own hormonal signals.
Is it serious?
In the large majority of cases, a fibroadenoma is harmless. The ordinary kind, called a simple fibroadenoma, does not meaningfully raise your future breast cancer risk. A smaller subset, called complex fibroadenomas (they contain cysts, calcifications, or certain cell changes), carry a slight increase in risk, which is why a pathologist's note of "complex" may lead your doctor to suggest closer monitoring.
The features radiologists do take seriously are change and atypia: a lump that is growing quickly, has irregular or spiky margins, or looks different from a classic fibroadenoma. One particular look-alike, a phyllodes tumor, can grow rapidly and behave differently, so a fibroadenoma that suddenly enlarges is worth re-evaluating promptly. None of this is a reason to panic. It simply means the finding gets checked rather than ignored.
Symptoms
Many fibroadenomas cause no symptoms at all and are discovered incidentally during imaging done for another reason. When you can feel one, it typically has a distinctive character: a firm but rubbery, smooth, well-rounded lump that moves easily under your fingers. That mobility is why it is sometimes nicknamed a "breast mouse." It is usually painless, though some women notice mild tenderness that fluctuates with their menstrual cycle. A lump that is hard, fixed in place, or associated with skin dimpling or nipple changes is a different picture and should be evaluated without delay.
How is it diagnosed and followed up?
Diagnosis combines a clinical exam with imaging: ultrasound for younger, denser breasts, and mammography for women over 40 or as a complement. When the appearance is classic and you are young, doctors often choose active surveillance: a repeat ultrasound in about 6 months, then at longer intervals, to confirm the lump is stable. Stability over time is itself strong reassurance.
Sometimes there is genuine uncertainty: atypical features, rapid growth, or a lump that can be felt but does not look classic. In that case, a core-needle biopsy is the next step. It removes a small tissue sample so a pathologist can confirm the diagnosis under the microscope. This is the same careful workflow used for other common findings women encounter, such as an ovarian cyst on ultrasound: image, characterize, and only intervene when the features warrant it.
Treatment options
There is no single "correct" treatment, because most fibroadenomas do not need any. The realistic options are:
- Watchful waiting: the default for a small, classic, stable fibroadenoma. Many shrink or stay quiet for years.
- Minimally invasive removal: vacuum-assisted excision or cryoablation (freezing) for lumps that are bothersome but clearly benign.
- Surgical removal (lumpectomy): considered for large (typically over 2–3 cm), growing, painful, or distorting lumps, or when you simply prefer it gone for peace of mind.
The choice depends on the lump's size and behavior, your symptoms, and your own preference. There is no medication that reliably dissolves a fibroadenoma, and removing one does not stop new ones from forming elsewhere.
Why a second read can help
Breast imaging is one of the areas where a careful, expert read matters most. The difference between BI-RADS 3 and BI-RADS 4, or between a classic fibroadenoma and a subtle look-alike, changes whether you watch or biopsy. If you want added confidence in how your ultrasound or mammogram was interpreted, DocOrbit offers an expert second read of your images that you can share directly with your own doctor. It is a way to ask "did anyone miss anything, and is watchful waiting really the right call?" before you decide. The same reasoning applies to getting a second radiological opinion for any worrying finding.
Is a fibroadenoma cancer?
No. A fibroadenoma is a benign (non-cancerous) breast lump made of normal glandular and connective tissue. It is the most common solid breast lump in younger women. A radiologist still confirms the benign features on imaging, and sometimes a needle biopsy is done to be certain, but a typical fibroadenoma is not cancer.
Do fibroadenomas need to be removed?
Most do not. When a lump has classic benign features and stays stable, doctors usually just watch it with periodic imaging. Removal is considered if it is large, growing, painful, distorting the breast, or if the diagnosis is uncertain. The decision is shared between you and your doctor.
Can a fibroadenoma turn into breast cancer?
A simple fibroadenoma very rarely turns into cancer and does not meaningfully raise your overall breast cancer risk. Complex fibroadenomas carry a slight increase in risk, which is why your doctor may recommend closer follow-up for those. Any new growth or change in features is checked carefully.
Why do fibroadenomas develop?
The exact cause is not fully understood, but fibroadenomas are sensitive to the hormone estrogen. That is why they are most common during the reproductive years, can grow during pregnancy or with hormone therapy, and often shrink after menopause. They are not caused by anything you did wrong.
Will my fibroadenoma go away on its own?
Some do. A portion of fibroadenomas stay the same size for years, some grow slowly, and a meaningful number shrink or disappear over time, especially after menopause. Because behavior varies, the usual approach for a newly found lump is short-interval imaging to see which way it is trending.
Key takeaways
- A fibroadenoma is the most common benign breast lump in younger women. It is not cancer.
- On ultrasound it looks oval, smooth-edged, and wider-than-tall; radiologists grade their concern with BI-RADS.
- They are hormonally driven, so they can grow in pregnancy and shrink after menopause.
- Most need only periodic imaging; removal is reserved for large, growing, symptomatic, or uncertain lumps.
- Any rapid growth or atypical feature should be re-checked promptly. That is caution, not cause for alarm.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.