Your doctor hands you a referral for a thyroid uptake scan, and later the report comes back describing your nodule as hot or cold. Those words sound dramatic, but they are simply a physicist's shorthand for how active a piece of thyroid tissue is. Here is what a thyroid scan actually measures, what hot and cold really mean, and why a cold nodule is not the alarming verdict the internet makes it out to be.
What a thyroid uptake scan actually is
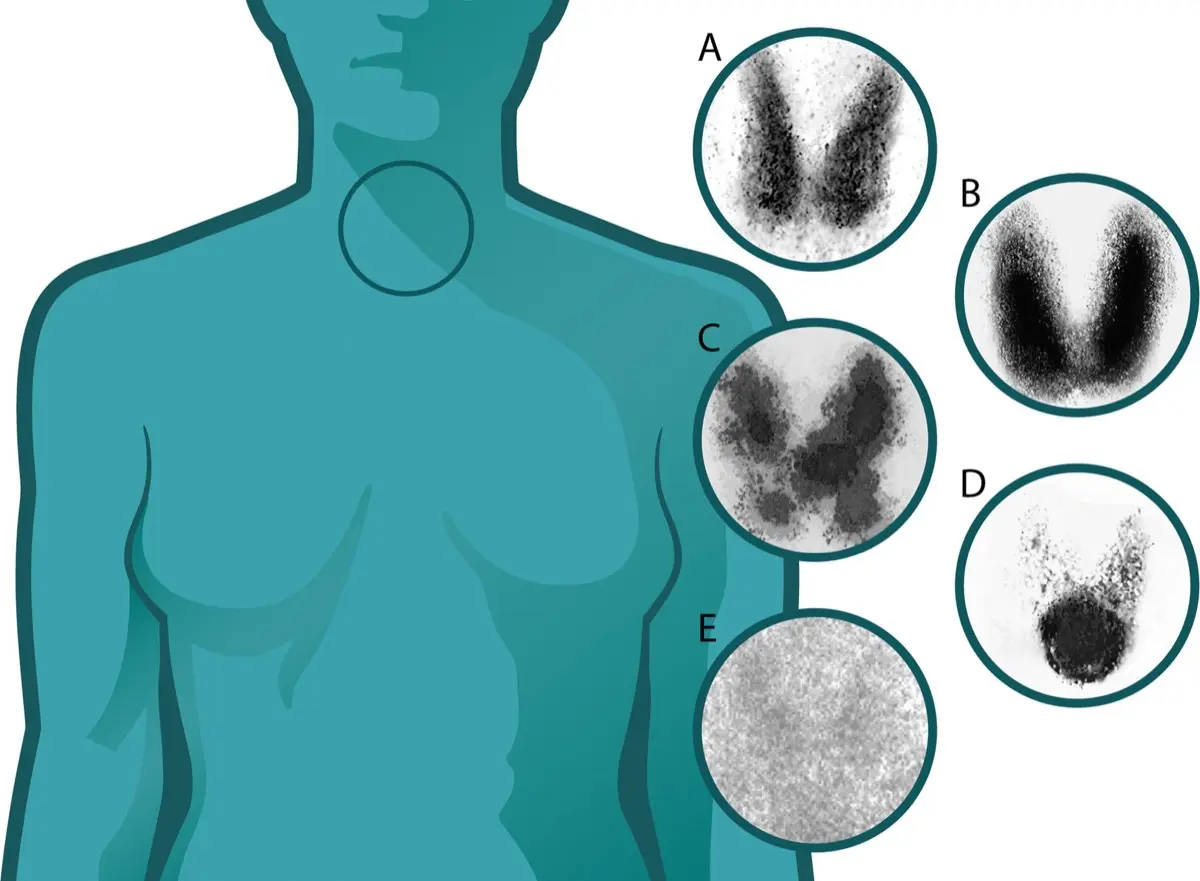
A thyroid uptake scan, also called thyroid scintigraphy, is a nuclear medicine test. You are given a small amount of a radioactive tracer, usually radioactive iodine (I-123) or technetium (Tc-99m), which the thyroid absorbs the same way it absorbs the iodine in your diet. A special camera then measures where the tracer collects. The result is a map of function, not just anatomy: it shows which parts of the gland are working hard and which are quiet.
This is what makes it different from the ultrasound most people have first. An ultrasound is a picture of structure, showing the size, borders, and internal texture of a nodule. A scan is a picture of activity. If you want the structural side of the story, our explainer on the thyroid nodule on ultrasound covers what the sonographer is looking for.
Hot, warm, and cold: what the words mean
Radiologists describe nodules by how much tracer they take up compared with the normal thyroid tissue around them:
- Hot (hyperfunctioning) — the nodule takes up more tracer than the rest of the gland. It is overactive and often makes extra thyroid hormone.
- Warm (indeterminate) — the nodule takes up about the same amount as normal tissue. It functions along with the rest of the gland.
- Cold (hypofunctioning) — the nodule takes up less tracer than the surrounding tissue. It is quieter on the scan.
The reassuring headline: hot nodules are almost never cancer. When a nodule is busy pumping out hormone, it is behaving like normal thyroid tissue on overdrive, and that behavior is overwhelmingly benign. Cold nodules get more attention, but even most of those turn out to be benign once fully worked up.
Why your doctor ordered the scan
An uptake scan is not part of the routine work-up for every nodule. It earns its place mainly when a blood test shows an overactive thyroid, that is, a low TSH with high thyroid hormone levels. In that situation the scan answers a specific question: is a single hot nodule causing the overactivity, is the whole gland overactive (as in Graves disease), or are there several hot areas (a toxic multinodular goiter)? The pattern changes what happens next.
Common reasons a scan is requested include:
- Blood tests suggesting hyperthyroidism (low TSH)
- Planning radioactive iodine treatment and estimating the dose
- Sorting out a multinodular goiter, where several nodules coexist
- Investigating a lump in the neck when hormone levels are abnormal
Is it serious?
For most people, the answer is reassuring. A hot nodule points toward an overactive but benign process that is very treatable. A cold nodule is the one specialists evaluate more carefully, not because it is likely to be cancer, but because a small minority of cold nodules can be, so it is worth the extra look. That extra look usually means an ultrasound and, depending on the features, a fine-needle aspiration biopsy to sample the cells directly.
What the scan cannot do is diagnose cancer by itself. It measures function, and function alone does not confirm or rule out a malignancy. That is why the scan is one instrument in an orchestra of tests, blood work, ultrasound, and sometimes biopsy, rather than the final word.
Symptoms that may go with the finding
Many nodules cause no symptoms at all and are found by accident. When symptoms do appear, they usually track with hormone levels rather than with the scan pattern itself. An overactive thyroid can bring a racing heartbeat, unexplained weight loss, heat intolerance, tremor, anxiety, or trouble sleeping. A large nodule of any type can sometimes be felt as a lump or cause a sensation of pressure when swallowing. None of these on their own tell you whether a nodule is hot or cold; only the scan and blood tests do that.
How it is followed up and treated
Treatment depends far more on function and biopsy results than on the scan label alone. A benign, quiet cold nodule may simply be watched with periodic ultrasound. A hot nodule causing hyperthyroidism has several well-established options: antithyroid medication, radioactive iodine to shrink the overactive tissue, or surgery in selected cases. Radioactive iodine treatment is closely related to the scan itself, because the same appetite for iodine that lit the nodule up is what lets the treatment target it.
If a biopsy raises concern, or a cold nodule has worrying ultrasound features, the conversation shifts toward surgery. But for the average person leaving the nuclear medicine department, the realistic path is monitoring or a straightforward, effective treatment, not an emergency.
Why a second read can help
Nuclear medicine images are interpreted alongside your blood work, your ultrasound, and your symptoms, and reasonable specialists can weigh those pieces differently, especially in a multinodular gland where hot and cold areas sit side by side. An independent second read can confirm the pattern, double-check that the right nodule is being blamed for an overactive thyroid, and give you a clear summary to bring to your endocrinologist. DocOrbit offers exactly that: a subspecialty-matched second opinion you can share with your own doctor. If you are weighing whether it is worth it, our guide on when to get a second radiological opinion walks through the situations where it changes decisions. For the closely related PET world, see our explainer on hypermetabolic uptake and SUV on PET-CT.
Is a cold thyroid nodule always cancer?
No. Most thyroid nodules are cold, meaning they take up little tracer, and the large majority of cold nodules are still benign. Cold simply means the nodule is less active than the surrounding gland, which is why it is usually evaluated further with ultrasound and sometimes a needle biopsy rather than assumed to be cancer.
Is a thyroid uptake scan safe?
Yes. The amount of radioactive tracer used is small and comparable to many routine imaging tests. The tracer clears from your body within a day or two. The main precaution is that pregnant and breastfeeding patients usually avoid it, so tell your doctor if either applies to you.
What is the difference between a hot and a cold thyroid nodule?
A hot nodule takes up more tracer than the rest of the thyroid and is overactive, producing extra hormone. A cold nodule takes up less tracer and is underactive on the scan. Hot nodules are almost always benign, while cold nodules are usually benign but are checked more carefully.
Why did my doctor order a thyroid scan instead of an ultrasound?
The two tests answer different questions. An ultrasound shows the size, shape, and structure of a nodule, while an uptake scan shows how active it is. A scan is most useful when your blood test shows an overactive thyroid, because it can pinpoint whether one hot nodule or the whole gland is responsible.
Do I need to stop any medications before a thyroid uptake scan?
Sometimes. Thyroid medication, iodine-containing supplements, and recent CT scans with iodinated contrast can affect the result. Your care team will tell you what to pause and for how long, so always share your full medication and recent-scan history before the appointment.
Key takeaways
- A thyroid uptake scan measures function, how active tissue is, not just its shape.
- Hot nodules are overactive and almost always benign; cold nodules are quieter and usually benign but checked more closely.
- The scan is most useful when blood tests show an overactive thyroid, and it is only one piece of the diagnosis alongside ultrasound and biopsy.
- Most people face monitoring or an effective, well-established treatment, not an emergency.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.