Seeing the words "ovarian cyst" on an ultrasound report can be unsettling, especially when the report lists a size in centimeters and a few unfamiliar terms. The reassuring truth is that ovarian cysts are one of the most common findings in women of reproductive age, and the large majority are completely harmless: fluid-filled sacs that come and go with the menstrual cycle. This guide explains what the finding means, what causes cysts, when they are simply incidental, and the specific features that make doctors want a closer look.
What "ovarian cyst" means
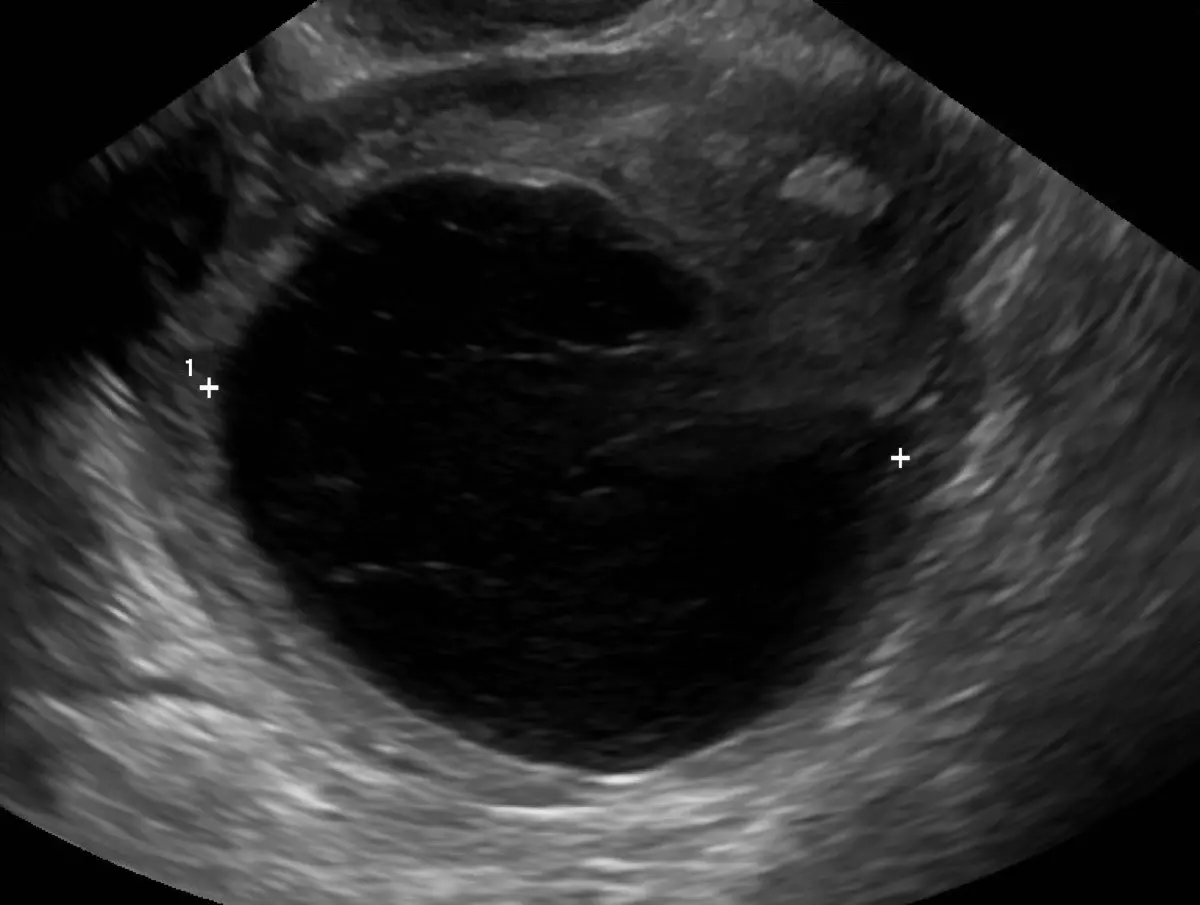
An ovarian cyst is a fluid-filled (or sometimes partly solid) sac on or within an ovary. Ultrasound is the first and best tool for looking at the ovaries, usually performed two ways: across the lower abdomen (transabdominal) and, for a clearer view, with a small probe inside the vagina (transvaginal). On the screen, a typical cyst appears as a dark, round pocket of fluid against the speckled background of ovarian tissue.
Radiologists describe a cyst by a handful of features that together tell most of the story:
- Size: measured in three dimensions or as a single largest diameter. Many functional cysts are only a few centimeters.
- Contents: clear fluid (anechoic) is reassuring; internal echoes, debris, or septations (thin internal walls) are described in more detail.
- Walls: thin and smooth is typical of a simple cyst; thick or irregular walls draw more attention.
- Solid areas and blood flow: solid nodules or internal blood flow on Doppler are the features doctors weigh most carefully.
Reports may use related phrases such as "simple adnexal cyst," "functional cyst," "hemorrhagic cyst," or "complex cyst," each pointing to a different appearance rather than a different level of danger.
Common causes and types
Most cysts are a normal byproduct of how the ovaries work. Each month an ovary grows a follicle that releases an egg; the machinery behind that process is the source of the most common cysts:
- Functional cysts: follicular cysts (a follicle that keeps growing instead of releasing) and corpus luteum cysts (the structure left after ovulation). These are the everyday cysts that resolve on their own.
- Hemorrhagic cysts: a functional cyst that has bled internally. They can look complex on ultrasound but are usually benign and settle over a few weeks.
- Dermoid cysts (teratomas): benign cysts that can contain fat, hair, or other tissue, with a characteristic look on imaging.
- Endometriomas: cysts related to endometriosis, often described as having uniform low-level internal echoes.
- Cystadenomas: benign growths from the surface of the ovary that can become larger.
Most ovarian cysts are picked up by chance and turn out to be benign, just like many other incidental imaging findings, from a lung nodule on a CT scan to changes in another organ.
Is it serious?
For most women the honest answer is "almost certainly not." What matters is not the word "cyst" but the cyst's appearance and your stage of life. A few useful distinctions:
- A simple cyst with thin walls and clear fluid in a menstruating woman is reassuring and very often disappears on its own.
- Complex features such as solid parts, thick or irregular walls, internal blood flow, or multiple septations prompt closer evaluation, though many complex-looking cysts are still benign.
- A cyst in a postmenopausal woman is taken a little more seriously, because functional cysts are not expected after menopause.
- Sudden, severe pelvic pain alongside a known cyst can signal a rupture or ovarian torsion (a twisted ovary) and deserves prompt medical attention.
To make these judgments consistent, radiologists increasingly use the ACR's O-RADS system, which scores an ovarian cyst from almost-certainly-benign to high-risk and suggests the matching next step. If your report mentions an O-RADS number, it is simply this risk-stratification score.
Symptoms
Many ovarian cysts cause no symptoms at all and are found incidentally during a scan done for another reason. When symptoms do occur, they tend to reflect the cyst's size or behavior rather than danger, and may include:
- Pelvic discomfort or a dull ache on one side.
- Bloating or a feeling of fullness in the lower abdomen.
- Changes around the menstrual cycle, including pain near ovulation.
- Sudden sharp pain, which can occur if a cyst ruptures or the ovary twists. This is a reason to seek care promptly.
Because so many cysts are silent, the absence of symptoms is reassuring rather than worrying.
How it is diagnosed and followed up
Ultrasound usually answers most of the question on its own. The next steps depend on the cyst's appearance and your age:
- Watchful waiting: for a simple cyst, a repeat ultrasound in six to twelve weeks often shows it has shrunk or vanished.
- MRI: when a cyst is large or complex, pelvic MRI can characterize its contents far more precisely than ultrasound.
- Blood tests: markers such as CA-125 may be checked in specific situations, interpreted carefully because many benign conditions can raise them.
- Specialist referral: cysts with concerning features are reviewed by a gynecologist, and risk scores help decide who needs it.
The right follow-up is individual: cadence and testing vary by patient, and your own doctor knows your symptoms and history. Most simple cysts need nothing more than a single follow-up scan for reassurance.
Treatment options
Treatment is matched to the cyst, not to the label. Common approaches include:
- Observation: the default for simple, small cysts, which usually resolve without any intervention.
- Pain relief: simple measures for the discomfort of a cyst or a manageable rupture.
- Hormonal contraception: sometimes used to reduce the formation of new functional cysts, though it does not shrink an existing one.
- Surgery: reserved for large, persistent, or symptomatic cysts, or those with features that warrant removal, often done with minimally invasive (laparoscopic) techniques.
Why a second read can help
The line between a "simple" and a "complex" cyst, and the O-RADS category that follows from it, comes down to careful interpretation of walls, septations, solid areas, and Doppler flow. Two readers can occasionally describe the same cyst differently, and that difference can change whether you are watched or sent for more tests. DocOrbit provides an expert second-opinion radiology report you can share with your own doctor. It is useful when a report is ambiguous, when a cyst sits in the borderline zone, or when you simply want the confidence that comes with a careful second look before any decision.
Are ovarian cysts dangerous?
Most ovarian cysts are not dangerous. The large majority are simple, fluid-filled functional cysts that form as a normal part of the menstrual cycle and disappear on their own within one to three cycles. A small fraction have features that need closer attention, such as rapid growth, solid areas, or worrying blood-flow patterns. Those are the ones doctors follow more carefully. The cyst's appearance on ultrasound, not just its presence, is what guides how seriously to take it.
Can an ovarian cyst go away on its own?
Yes. Simple functional cysts very commonly resolve without any treatment, often within one to three menstrual cycles. This is why doctors frequently recommend a repeat ultrasound in six to twelve weeks rather than rushing to intervene. Cysts that persist, grow, or look complex are the ones that may need further evaluation.
Does an ovarian cyst mean cancer?
In the vast majority of cases, no. Ovarian cysts are extremely common and the overwhelming majority are benign, especially in women who are still menstruating. Certain features do raise concern: solid components, thick irregular walls, internal blood flow, or a cyst that grows in a postmenopausal woman. These prompt additional imaging or blood tests. A simple cyst with smooth, thin walls and clear fluid is reassuring.
When does an ovarian cyst need surgery?
Surgery is usually reserved for cysts that are large, persistent, causing significant symptoms, or showing features that could suggest something other than a simple cyst. Sudden severe pain from a ruptured cyst or a twisted ovary (torsion) can also require urgent surgery. Most small, simple cysts never need an operation and are simply watched until they resolve.
Key takeaways
- Ovarian cysts are very common, and most are simple functional cysts that resolve on their own within a few cycles.
- What determines how seriously a cyst is taken is not its presence but its appearance on ultrasound: the walls, contents, solid areas, and blood flow.
- Simple cysts in menstruating women are reassuring; complex features or a cyst after menopause prompt closer evaluation.
- Follow-up varies by patient, and a clear second read can help when a cyst sits in the borderline zone.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.