If your X-ray or MRI report mentions "osteoarthritis", "degenerative joint disease", or "joint-space narrowing", and especially if someone used the words "bone on bone", it is natural to picture the worst. Here is the reassuring truth: osteoarthritis is the single most common joint finding in the world, most people who have it stay active for years without surgery, and how your joint looks on a scan does not decide how much it will hurt or how you will be treated. This article explains what the finding means, why the picture and the pain so often disagree, and what actually helps.
What osteoarthritis means on a scan
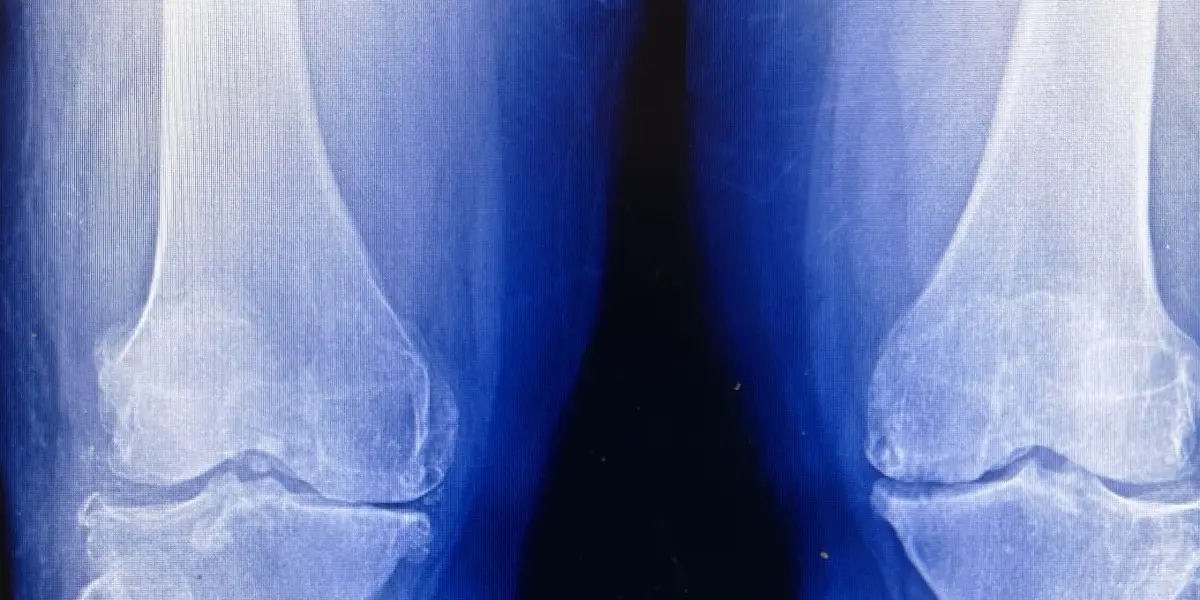
A healthy joint has a smooth layer of cartilage capping each bone end, so the bones glide over one another with almost no friction. Osteoarthritis is the gradual thinning and roughening of that cartilage, along with the changes the bone makes in response. On an X-ray the cartilage itself is invisible, so radiologists judge it indirectly by the gap between the bones, and they look for four classic features:
- Joint-space narrowing — the gap looks smaller because the cartilage cushion has thinned. This is the finding behind the phrase "bone on bone".
- Osteophytes — small bony spurs that grow at the joint margins as the bone reshapes.
- Subchondral sclerosis — a bright, dense rim of bone just beneath the worn surface.
- Subchondral cysts — small fluid-filled pockets in the bone near the joint.
An MRI can show the cartilage directly and also picks up bone-marrow changes, small effusions, and meniscal or ligament wear, which is why a knee MRI sometimes describes degeneration that a plain X-ray does not fully capture. Both are just describing the same underlying process at different resolutions.
How osteoarthritis is graded
Many reports assign a grade, most often using the Kellgren-Lawrence scale, which runs from 0 (normal) to 4 (severe). Grade 1 means doubtful narrowing with a tiny spur; grade 2 is definite spurs with possible narrowing; grade 3 is clear narrowing with multiple spurs and some bone change; grade 4 is marked narrowing, large spurs, and dense bone, the picture people call "bone on bone". The grade is a useful shorthand for what the radiologist sees, but it is not a verdict on your future. A higher grade does not automatically mean more pain, faster decline, or an inevitable operation.
Why the picture and the pain so often disagree
This is the most important thing to understand, and it surprises many patients. Study after study has found that the appearance of a joint on imaging and the amount of pain a person feels frequently do not match. Plenty of people have advanced-looking X-rays and only mild, occasional aches, while others with milder scans have more trouble. Pain in osteoarthritis is shaped by inflammation, the strength of the muscles around the joint, activity levels, body weight, sleep, and mood, none of which show up on the film. So a scary-sounding report paired with a joint that still lets you walk, climb stairs, and sleep is genuinely good news. Doctors treat the person in front of them, not the image.
Common causes and who gets it
Osteoarthritis usually comes from the ordinary accumulation of years of use, which is why it becomes far more common after middle age. Several things raise the odds or speed it up:
- Age — the strongest single factor.
- Extra body weight — every kilogram adds load to the knees and hips, and fat tissue also releases inflammatory signals.
- Previous injury — an old fracture, ligament tear, or meniscal tear can lead to arthritis in that joint years later.
- Repetitive heavy load — certain occupations and high-impact sport over decades.
- Genetics and joint shape — some families and some anatomies are simply more prone to it.
It most often affects the knees, hips, hands, and the spine. The same degenerative process in the spine is what a report may call degenerative disc disease, a close relative of the osteoarthritis seen in the limb joints.
Symptoms to expect
Typical osteoarthritis symptoms come and go and build slowly over years rather than suddenly. The usual pattern includes pain that is worse with activity and eases with rest, stiffness in the morning or after sitting that loosens within about half an hour, a grinding or clicking sensation, and sometimes mild swelling after a busy day. Many joints with early changes cause no symptoms at all. Signs that deserve a closer look, and a prompt call to your doctor, include a hot and markedly swollen joint, pain that wakes you every night, a joint that locks or gives way, or rapidly worsening pain, since these can point to inflammation or another problem beyond ordinary wear.
What actually helps
The foundation of osteoarthritis care is not medication or surgery, it is movement and load management, and the evidence here is strong. The measures that make the biggest difference for most people are:
- Exercise — strengthening the muscles around the joint and staying active is the most effective single treatment. It reduces pain and improves function, and the old fear that activity "wears the joint out faster" is not how it works.
- Weight management — losing even a modest amount of weight measurably lowers knee and hip load and eases symptoms.
- Pain relief — simple analgesics or topical anti-inflammatories used sensibly can keep you moving; your doctor will match these to your health.
- Injections — a corticosteroid injection can calm a painful flare in selected joints.
- Joint replacement — reserved for severe, function-limiting arthritis that has not responded to the above. Modern hip and knee replacements are among the most successful operations in medicine, but they are a last step, not a first one.
Why a second read can help
Because a joint's appearance and its symptoms so often diverge, the interpretation of an arthritis scan matters, and the same film can be framed as "reassuring wear" or "advanced disease" depending on who reads it and how the words land with an anxious patient. An independent expert read can confirm the grade, flag anything atypical for simple osteoarthritis, and put the findings in plain language. DocOrbit offers an expert second read of your imaging that you can share with your own doctor, which can be steadying when you are trying to decide whether an operation is really necessary yet. If you are weighing that choice, our guide on when to get a second radiological opinion walks through the situations where it helps most.
Does osteoarthritis on an X-ray mean I need a joint replacement?
No. The large majority of people with osteoarthritis on imaging are managed for years without surgery, using exercise, weight management, and pain relief. Joint replacement is considered only when pain and loss of function are severe and have not responded to those measures. The X-ray grade is one input, but the decision rests mostly on how much the joint affects your daily life.
What does bone-on-bone actually mean?
Bone-on-bone is a casual phrase for advanced joint-space narrowing, where the cartilage cushion has worn thin enough that the two bone ends sit very close together on the X-ray. It sounds dramatic, but it describes the picture, not your pain. Some people with a bone-on-bone X-ray have modest symptoms, while others with milder-looking scans hurt more, which is why doctors treat the person, not the film.
Why does my X-ray look bad but my knee does not hurt much?
This mismatch is common and well documented. Imaging severity and symptom severity often do not line up, because pain also depends on inflammation, muscle strength, activity, sleep, and other factors the X-ray cannot show. A worrying-looking film with mild symptoms is generally reassuring, not a reason to rush into treatment.
Is osteoarthritis the same as rheumatoid arthritis?
No. Osteoarthritis is a wear-related condition of cartilage and bone that usually affects a few weight-bearing or heavily used joints. Rheumatoid arthritis is an autoimmune disease that inflames the joint lining, often in a symmetric pattern across many small joints, and needs different treatment. Blood tests and the pattern of joints involved help tell them apart.
Can osteoarthritis be reversed or cured?
There is no treatment that regrows worn cartilage, so osteoarthritis cannot currently be reversed. It can, however, be managed very effectively. Many people keep their symptoms low and stable for years with strengthening exercise, weight control, and, when needed, medication or injections, and a joint replacement is a highly successful option if symptoms become severe.
Key takeaways
- Osteoarthritis on a scan describes worn cartilage and the bone's response to it; joint-space narrowing is the finding behind "bone on bone".
- Imaging severity and pain often do not match, so a worrying-looking film with mild symptoms is usually reassuring.
- Exercise and weight management are the most effective treatments; surgery is a last resort for severe, function-limiting disease.
- The grade on your report is a description, not a prediction of surgery or decline.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.