Few lines on a brain MRI report land harder than the word "meningioma" sitting next to "mass" or "lesion." If yours mentions one, here is the reassuring place to start: a meningioma is the most common tumor that forms in the head, the large majority are benign (non-cancerous) and slow-growing, and many are found by accident and never need more than a periodic scan. Below is what radiologists actually see, why these growths form, and what usually happens next.
What does "meningioma" mean?
A meningioma is a tumor that grows from the meninges, the thin protective layers that wrap around the brain and spinal cord, rather than from the brain tissue itself. Because it sits on the surface, pushing on the brain rather than growing inside it, radiologists call it an "extra-axial" mass. That single fact is a big part of why so many meningiomas are removable and well-behaved.
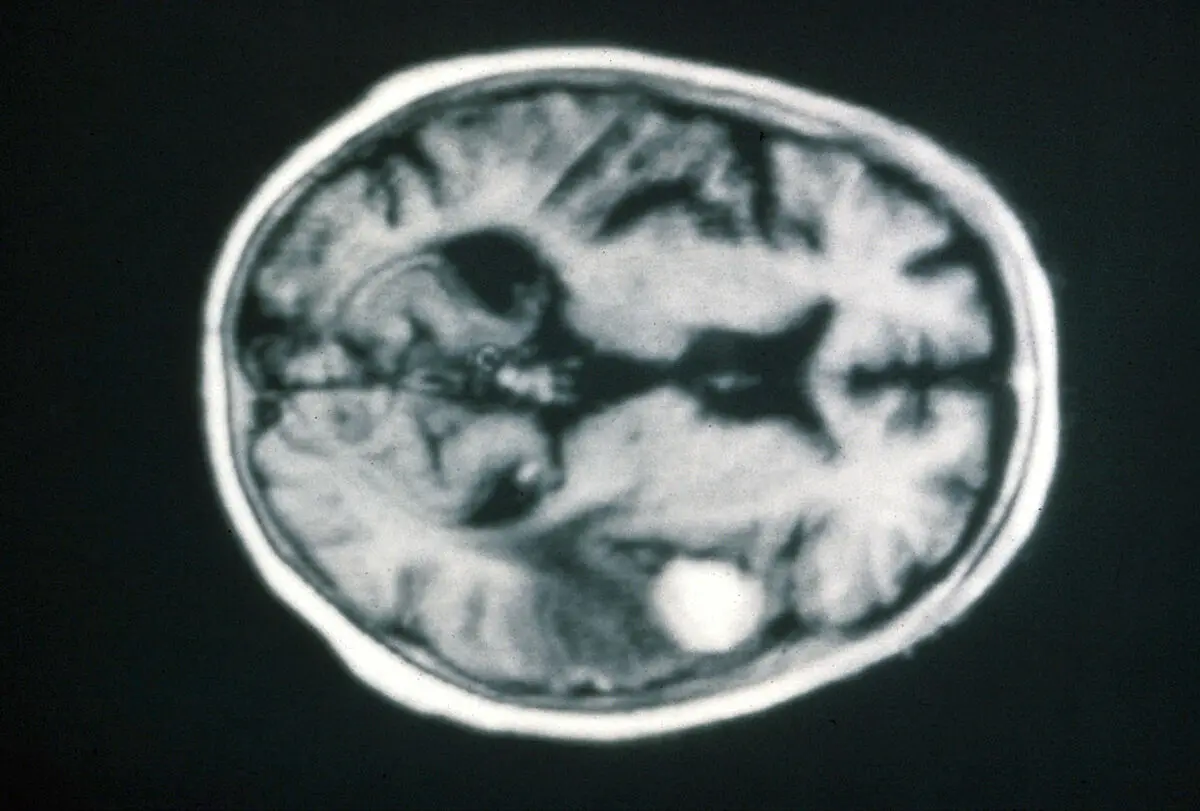
On an MRI with contrast, a meningioma has a fairly classic look. Radiologists tend to describe a handful of features:
- A dural-based mass, a well-defined, rounded growth attached by a broad base to the dura (the outer covering), the skull, or a membrane between brain regions.
- Bright, uniform enhancement, after contrast is given, the tumor lights up strongly and evenly.
- A "dural tail", a thin streak of enhancement trailing off along the dura beside the tumor, one of the hallmark signs.
- Associated changes, sometimes a little swelling (edema) in the nearby brain, or flecks of calcium within the tumor.
Meningiomas are also graded. The World Health Organization sorts them into three grades: grade 1 (benign, by far the most common), grade 2 (atypical), and grade 3 (anaplastic or malignant, which is rare). The grade, not the word "tumor", is what really shapes the outlook.
Common causes and risk factors
For most people there is no clear reason a meningioma formed, and nothing they did caused it. Still, a few factors are linked to a higher chance:
- Age, meningiomas become more common with age and are most often diagnosed in middle age and older.
- Female sex, they are roughly twice as common in women, and some carry hormone receptors, which is why they are watched a little more closely during pregnancy.
- Prior radiation to the head, earlier radiation therapy, sometimes decades before, is the best-established risk factor.
- Neurofibromatosis type 2, a rare inherited condition that predisposes to meningiomas, often more than one.
None of these guarantee a meningioma, and most people who develop one have none of them.
Is it serious?
For the large majority of people, a meningioma is a manageable finding rather than an emergency. Most are WHO grade 1, grow slowly over years, and may never cause a problem. Plenty are discovered incidentally, on a scan done for headaches, dizziness, or a head injury that turns out to be unrelated, and are simply watched.
What moves a meningioma up the priority list is its size, its location, and whether it is causing symptoms. A small tumor over a quiet part of the brain is very different from one pressing on the optic nerve, the brainstem, or a major vein. Rapid growth, significant surrounding swelling, or a higher grade (2 or 3) are the features that prompt more active treatment. These are the cases doctors act on deliberately, not with panic, but with a clear plan. A finding like this sits in different territory from an incidental note such as gliotic changes or age-related cerebral atrophy, which usually need no treatment at all.
Symptoms
Many meningiomas cause no symptoms whatsoever, which is exactly why so many are found by chance. When symptoms do appear, they depend almost entirely on where the tumor sits and what it presses against:
- Headaches, especially ones that are new or changing
- Seizures
- Gradual weakness or numbness on one side of the body
- Vision changes or loss of smell, when the tumor is near the relevant nerves
- Subtle shifts in memory, personality, or concentration with larger frontal tumors
Because these symptoms overlap with many ordinary conditions, the imaging always has to be read alongside your history and exam rather than on its own.
How it's diagnosed and followed up
MRI with contrast is the best test for finding and characterizing a meningioma; a CT scan can add detail about calcium or involvement of the skull. In many cases the appearance is typical enough that radiologists are confident without a biopsy.
For a small, symptom-free meningioma, the standard approach is often "watchful waiting", a repeat MRI in several months, then at widening intervals if it stays stable. This active monitoring lets doctors confirm the tumor is behaving as expected before considering anything more. The exact follow-up cadence varies by patient, size, and location, and is something your own neurologist or neurosurgeon tailors to your case.
Treatment options
Treatment is matched to the tumor and to you, not to the MRI alone. The main paths are:
- Observation, for small, asymptomatic, typical-looking meningiomas, monitoring with serial MRI is frequently all that is needed.
- Surgery, when a tumor causes symptoms, grows, or is large, surgical removal is the most definitive option, and for accessible grade 1 tumors it can be curative.
- Radiation therapy or stereotactic radiosurgery, for tumors that are hard to reach, left over after surgery, or in people for whom surgery is not ideal, focused radiation can control growth.
The right choice is a shared decision with a neurosurgeon and, often, a radiation oncologist, weighing the tumor's behavior against the risks of treating versus watching.
Living with the diagnosis
Seeing the word "tumor" on a brain scan is one of the most stressful things a report can say, and being told to "watch and wait" can feel counterintuitive, knowing something is there and simply living with it is genuinely hard. Yet for small, slow-growing meningiomas that watch-and-wait plan is a deliberate, safe choice that spares you the risks of an operation you may never need. Keeping your follow-up scans, managing any symptoms the way your doctor advises, and writing down your questions before appointments are the most practical ways to take back a sense of control.
Why a second read can help
A brain MRI that mentions a tumor is one of the most stressful reports a person can receive, and meningiomas sit on a wide spectrum, from a tiny incidental spot that only needs an annual scan to a tumor near a critical structure that changes the whole plan. Two radiologists can describe the same study in meaningfully different terms, and the difference between watching a tumor and treating it can hinge on subtle features. If your report leaves you unsure how worried to be, an expert second read can clarify the tumor's size, location, and likely grade. DocOrbit makes it straightforward to get a second opinion on your scan that you can share with your own doctor, the same reasoning behind getting a second radiological opinion for any consequential finding.
Is a meningioma a brain tumor or cancer?
A meningioma is a brain tumor in the broad sense, but it grows from the brain's covering layers rather than from brain tissue, and the large majority are benign, not cancer. Only a small fraction are atypical (grade 2) or malignant (grade 3). For most people, meningioma means a non-cancerous, slow-growing growth.
Are meningiomas dangerous?
Most meningiomas are not dangerous and grow so slowly they may never cause trouble. Whether one is concerning depends on its size, its location, and whether it presses on important structures, a small tumor over a quiet area is very different from one near the optic nerve or brainstem. Higher-grade or rapidly growing tumors are the ones doctors treat more actively.
Do all meningiomas need surgery?
No. Many small, symptom-free meningiomas are simply monitored with repeat MRI scans and never need surgery. Surgery is usually considered when a tumor causes symptoms, grows on follow-up, or is large. Radiation therapy is another option for tumors that are hard to reach or left over after surgery.
How fast does a meningioma grow?
Most benign (grade 1) meningiomas grow very slowly, often only a millimeter or two per year, and some do not measurably grow at all. This slow pace is why watchful waiting with periodic scans is a safe, common strategy. Higher-grade meningiomas grow faster, which is one reason follow-up imaging matters.
Can a meningioma cause headaches?
It can, but headaches have countless ordinary causes, and many people found to have a meningioma were scanned for a headache that turned out to be unrelated. When a meningioma does cause symptoms, they depend on its location and can include headaches, seizures, or focal weakness. Symptoms always need to be interpreted alongside the imaging, not from the scan alone.
Key takeaways
- A meningioma grows from the brain's protective covering, not from brain tissue, and the large majority are benign and slow-growing.
- Many are found by accident and cause no symptoms; size and location matter far more than the word "tumor."
- Watchful waiting with serial MRI is a standard, safe approach for small, asymptomatic tumors.
- Surgery or focused radiation is reserved for tumors that grow, cause symptoms, or are higher grade.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.