If your brain MRI mentions a "lacunar infarct," the word "infarct" can sound frightening. For many people, though, it describes an old, small area of damage deep in the brain that the body has long since adapted to. Lacunar infarcts are a specific type of small stroke, and on imaging they often turn up quietly, sometimes without the person ever knowing one happened. This guide explains what the term means, what causes these small strokes, when they matter, and how doctors typically follow them up.
What "lacunar infarct" means
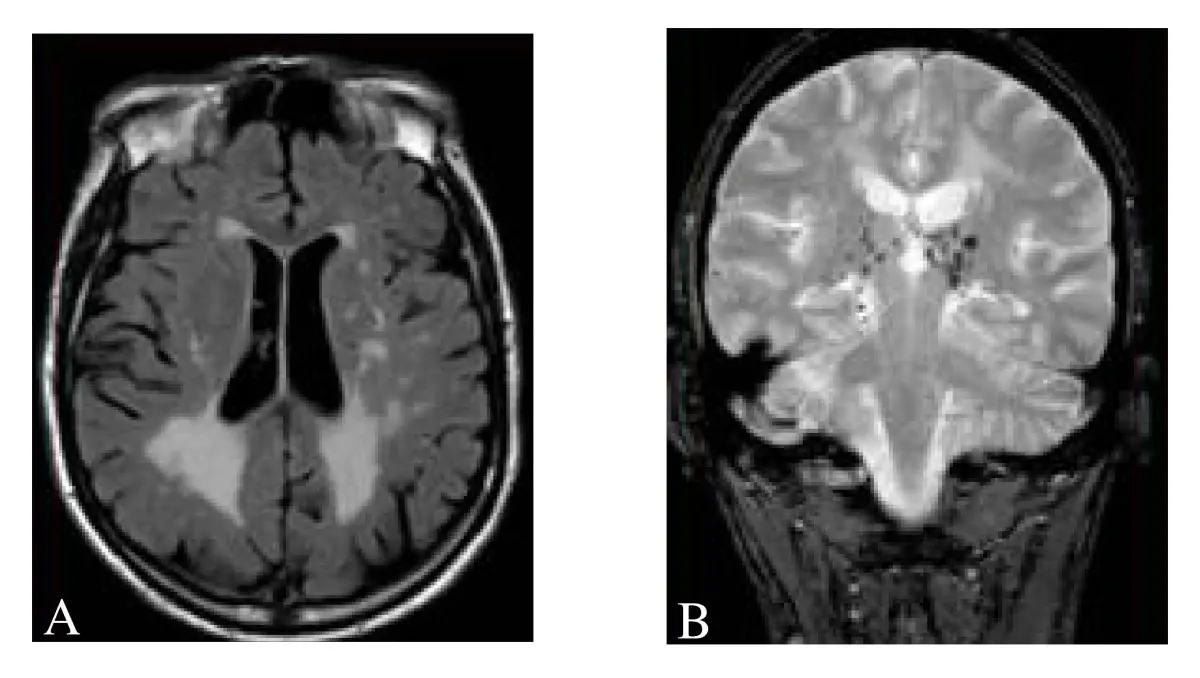
A lacunar infarct is a small area of brain tissue damage caused by blockage of one of the tiny arteries deep inside the brain. These arteries are only a fraction of a millimeter wide, yet they feed important deep structures including the basal ganglia, thalamus, internal capsule, and parts of the pons in the brainstem. When one of them closes off, the patch of brain tissue it supplied dies, and what remains is a small cavity or scar, usually 3 to 15 millimeters across. Radiologists call that little cavity a "lacune", from the Latin for "little lake".
On MRI, an old lacunar infarct looks like a small spot of fluid-density tissue in a deep, predictable location. Reports use phrases like:
- Lacunar infarct: the standard term.
- Old or chronic lacunar infarct: one that happened in the past, often without symptoms at the time.
- Lacune: older shorthand for the same finding.
- Acute lacunar infarct: a small stroke happening now, usually flagged by a special MRI sequence called diffusion-weighted imaging.
The word "old" or "chronic" matters. Chronic lacunes are imaging history. An acute lacunar infarct is described differently and is taken as an active stroke, even when symptoms are mild.
Common causes
Lacunar infarcts are the classic imaging signature of small vessel disease, which means long-term wear on the deep, tiny arteries of the brain. The most common drivers include:
- High blood pressure (hypertension): the single most important risk factor.
- Diabetes: sustained high blood sugar damages small vessel walls.
- High cholesterol: it accelerates plaque in small arteries.
- Smoking: both current and long-term past use.
- Age: small vessel disease accumulates over decades.
- Atrial fibrillation: an irregular heart rhythm that can throw small clots into the deep brain arteries.
These same factors drive other findings that often appear in the same report, such as chronic ischemic changes in the white matter and, over years, a degree of cerebral atrophy.
Is it serious?
A lacunar infarct is a real stroke. It is simply a small, deep one, and that carries different implications than the term "stroke" usually conveys. Many lacunar infarcts are found incidentally on a brain MRI ordered for something unrelated: a fall, dizziness, headache, or routine memory testing. People with these "silent" lacunes often had no recognized event.
Even a silent lacunar infarct is a marker of small vessel disease, and the factors that produced one tend to produce more if left unmanaged. The clinical weight depends on:
- Whether it caused symptoms: pure motor weakness, pure sensory loss, dysarthria, or a clumsy hand are classical "lacunar syndromes".
- How many are present: multiple lacunes, especially with extensive white-matter changes, raise the risk of step-wise cognitive decline.
- Whether it is acute: an acute lacunar infarct is a stroke that needs prompt evaluation, even if mild.
- The location: lacunes in the thalamus or brainstem can have outsized effects despite small size.
Symptoms
Many lacunar infarcts cause no symptoms at all. That is why they so often turn up as an incidental finding. When they do produce symptoms, the classical "lacunar syndromes" appear suddenly:
- Pure motor stroke: weakness on one side of the face, arm, and leg, without loss of feeling.
- Pure sensory stroke: numbness on one side of the body.
- Sensorimotor stroke: combined weakness and numbness on the same side.
- Ataxic hemiparesis: weakness on one side with clumsiness or balance trouble.
- Dysarthria-clumsy hand syndrome: slurred speech with a clumsy hand.
These symptoms suggest an active stroke and warrant urgent medical evaluation. By contrast, an old lacunar infarct identified on an MRI for chronic headache or routine workup is a finding, not an emergency.
How it is diagnosed and followed up
Lacunar infarcts are diagnosed on MRI. CT can show larger lacunes, especially old ones, but MRI is far more sensitive: diffusion-weighted imaging (DWI) shows acute strokes, and FLAIR sequences show old lesions.
When a lacunar infarct is found, the workup usually looks like this:
- Your doctor reviews the full vascular picture: blood pressure, blood sugar, cholesterol, and sometimes heart-rhythm monitoring for atrial fibrillation.
- A neurologist or primary care doctor decides whether further imaging is needed (vascular MRI or CT angiography of the neck and brain vessels).
- If there are symptoms, the workup is more urgent.
- For old, silent lacunes, the focus shifts to risk factor control, which is how new ones are prevented.
Routine follow-up imaging is not always needed. It is usually arranged when symptoms change, when the burden of small vessel disease is heavy, or when a doctor wants to track progression over time.
Treatment options
Treatment is aimed less at the existing lacune (which cannot be reversed) and more at preventing the next one. Common approaches include:
- Blood pressure control: the single most effective intervention.
- Antiplatelet therapy: usually low-dose aspirin or clopidogrel, when prescribed by a doctor.
- Statin therapy: for cholesterol, and often used in stroke patients regardless of starting cholesterol level.
- Diabetes management: keeping blood sugar in target ranges.
- Treating atrial fibrillation: anticoagulation when appropriate.
The specific medication mix depends on the individual. Your doctor weighs your other conditions, bleeding risk, and overall picture.
Lifestyle changes
The same lifestyle changes that protect the heart protect the brain's small vessels:
- Quitting smoking: the most impactful single change.
- A Mediterranean-style diet: vegetables, fruit, fish, olive oil, whole grains.
- Regular aerobic exercise: typically 150 minutes a week of moderate activity.
- A healthy weight and limiting alcohol.
- Treating sleep apnea if present, because it raises blood pressure overnight.
Progress is measured in years. Someone who controls blood pressure consistently for a decade has measurably less new small vessel damage than someone whose blood pressure runs uncontrolled.
Why a second read can help
Reading the difference between a routine, age-related lacune and one that demands a closer vascular workup is judgment work that varies between radiologists. A second read can confirm the lesion is genuinely old and lacunar rather than a different small finding, count any additional lacunes accurately, and put the overall small vessel disease burden into a clear picture you can show your own physician. DocOrbit provides an expert second-opinion radiology report you can share with your doctor. It can help when you want a clearer view of how much small vessel disease is present and whether it changes the next step in your care.
Is a lacunar infarct a stroke?
Yes. A lacunar infarct is a type of ischemic stroke that occurs in one of the brain's tiny deep arteries. It differs from the picture most people have of a stroke because lacunes are small, often silent, and frequently discovered long after they happened. Even when silent, they share the same underlying disease process as larger strokes, which is why doctors treat them as a warning sign rather than ignore them.
Can a lacunar infarct go away?
No. Once brain tissue is lost to a lacunar infarct, that small cavity remains visible on future MRIs. What can change is whether new lacunes appear, and that depends largely on how well the underlying small vessel disease is managed. Stable imaging over years, with no new lacunes, is itself a meaningful sign of good control.
Are lacunar infarcts dangerous?
A single small, silent lacunar infarct is usually not dangerous on its own, but it signals small vessel disease that deserves attention. The real concern is what comes next. Repeated lacunes can accumulate and contribute to cognitive decline, gait disturbance, or, less commonly, a clinically obvious stroke. Treating the underlying risk factors is what changes that trajectory.
What lifestyle changes prevent more lacunar infarcts?
The biggest levers are blood pressure control, stopping smoking, treating diabetes and high cholesterol, exercising regularly, and eating a Mediterranean-style diet. Sleep, stress management, and limiting alcohol matter too. These are the same vascular risk factors that protect the heart, and the brain's small vessels respond to them across years rather than weeks.
Key takeaways
- A lacunar infarct is a small, deep stroke in one of the brain's tiny arteries. On MRI it usually appears as a small cavity.
- Many are silent and found incidentally; even silent ones signal small vessel disease worth treating.
- High blood pressure is the most important driver. Quitting smoking, managing diabetes and cholesterol, exercising, and a Mediterranean-style diet slow how fast new ones appear.
- Old lacunes cannot be reversed. Preventing new ones, however, responds well to consistent care.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.