Seeing "disc herniation" or "herniated disc" on an MRI report can be alarming, especially if you went in for back or leg pain. Here is the reassuring truth: herniated discs are extremely common, they show up on the scans of many people who have no pain at all, and the large majority get better without surgery. This article explains what the finding means, why it happens, what symptoms to look for, and how it is usually treated.
What does disc herniation mean on MRI?
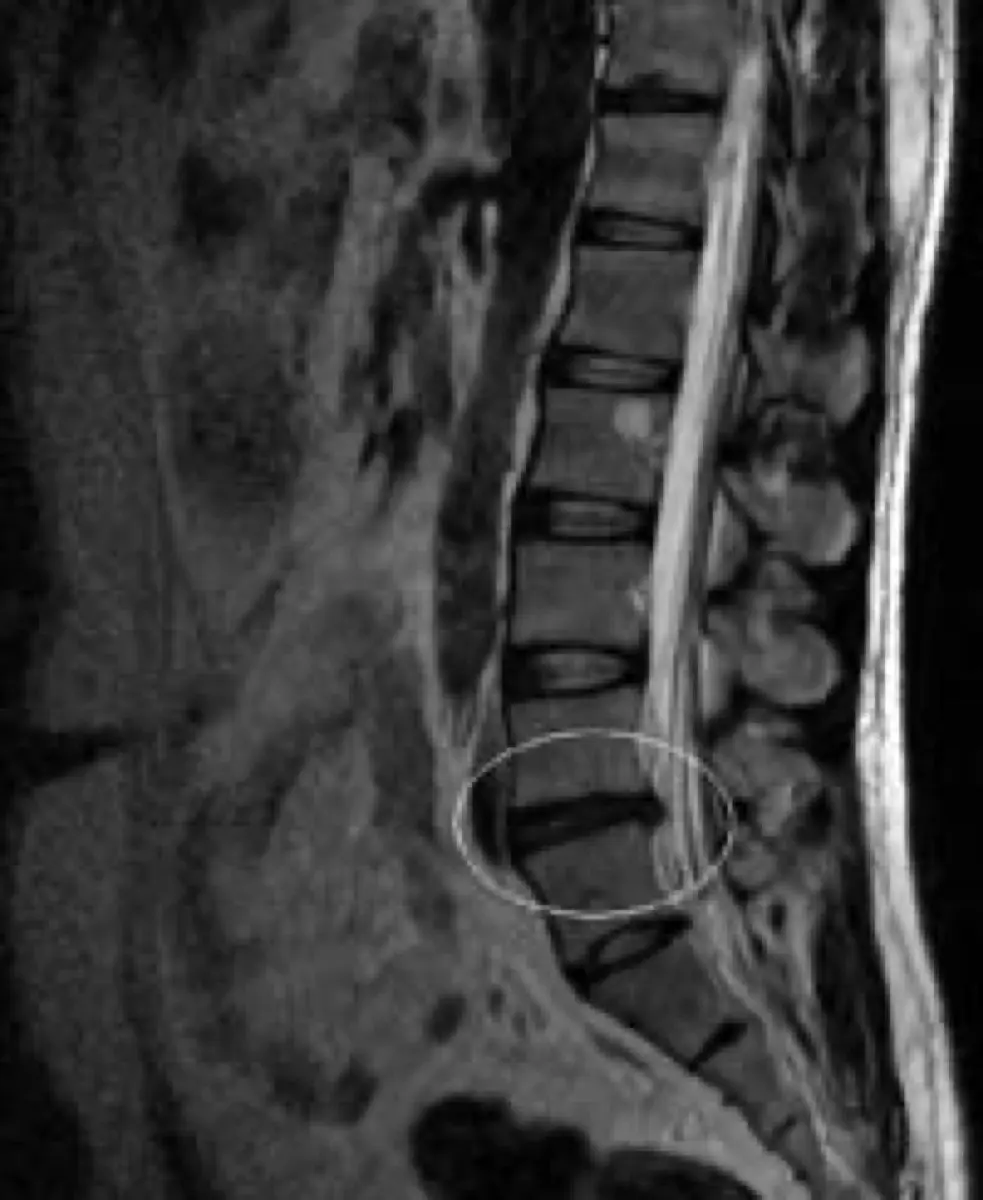
Between each pair of spinal bones (vertebrae) sits a cushion called an intervertebral disc. Each disc has a tough outer ring and a soft, gel-like center. A herniation happens when some of that inner material pushes through a weak spot or tear in the outer ring. On MRI, the radiologist sees this displaced material extending beyond the normal disc margin, sometimes toward the spinal canal or the channel where a nerve root exits.
You may see several different words used for the same general process, ranging from mild to more pronounced:
- Disc bulge — the disc extends outward broadly with the outer wall still intact; often a normal age-related change.
- Protrusion — a focal herniation where the base is wider than the part that sticks out.
- Extrusion — disc material pushes further out, with the protruding part wider than its neck.
- Sequestration — a fragment breaks away from the parent disc entirely.
The report often names the level too, such as L4–L5 or L5–S1 in the lower back, or C5–C6 in the neck. These are simply the locations between vertebrae where the herniation sits.
Common causes
Most herniations are not caused by a single dramatic injury. They usually reflect the gradual wear that affects everyone's spine over time, sometimes nudged over the edge by an everyday movement.
- Age-related disc dehydration and weakening of the outer ring
- Repetitive bending, lifting, or twisting
- A single heavy or awkward lift
- Prolonged sitting and deconditioning of the core muscles
- Smoking, which reduces disc nutrition
- Genetics — some people simply have discs that wear faster
Is a herniated disc serious?
For most people, a herniated disc is a painful but self-limiting problem rather than a dangerous one. Studies that scan people with no back pain at all find disc herniations in a meaningful fraction of them, which is exactly why the MRI finding has to be read alongside your symptoms. A herniation that matches your pain pattern is meaningful; an incidental one that does not may need no action.
There are a few situations doctors treat with more urgency: a fragment compressing a nerve enough to cause progressive weakness, or — rarely — pressure on the bundle of nerves at the base of the spine. That last scenario, called cauda equina syndrome, can cause numbness around the groin and loss of bladder or bowel control, and it needs emergency evaluation. These red-flag cases are uncommon, but they are the reason the symptoms below matter as much as the scan.
Symptoms
Symptoms depend on whether the herniation is touching a nerve and which one. Many herniations cause nothing at all. When they do cause trouble, common patterns include:
- Pain radiating down one leg (sciatica) from a lower-back herniation, or down an arm from a neck herniation
- Tingling, pins-and-needles, or numbness in a specific area
- Muscle weakness in the affected limb
- Pain that worsens with sitting, coughing, sneezing, or bending forward
Because the nerves that travel down the leg and arm start in the spine, these findings sit at the crossroads of orthopedics and neurology — a reason careful interpretation matters, as we discuss in why a second opinion on a neurological diagnosis can be a lifesaver.
How is it diagnosed and followed up?
MRI is the best test for showing soft tissues like discs and nerves, which is why it is the standard imaging study when symptoms point to a herniation. That said, doctors do not treat the picture alone — they correlate it with your history and a physical exam that tests reflexes, strength, and sensation. If the herniation explains your symptoms, follow-up is mostly clinical: how you feel over the coming weeks usually guides the plan more than a repeat scan. Repeat imaging is generally reserved for symptoms that worsen or fail to improve, or before a planned procedure.
Treatment options
The encouraging headline is that most herniated discs are managed without surgery. A typical pathway looks like this:
- Stay gently active — prolonged bed rest tends to slow recovery rather than speed it.
- Pain relief — over-the-counter anti-inflammatories or other medications your doctor recommends to get you through the worst weeks.
- Physical therapy — targeted exercises to ease nerve irritation, build core support, and improve movement patterns.
- Injections — in selected cases, an epidural steroid injection can reduce inflammation around an irritated nerve.
- Surgery — reserved for severe or progressive nerve compression, or pain that does not respond to months of conservative care. Procedures like microdiscectomy relieve pressure on the affected nerve.
Time itself does a lot of the work here. Herniations often shrink as the body reabsorbs the displaced material, and many people feel substantially better within six to twelve weeks.
Lifestyle changes that help
Day-to-day habits influence both recovery and the odds of a future flare. Practical steps that tend to help include staying physically active with low-impact exercise like walking or swimming, building core and back strength, lifting with your legs rather than your back, taking breaks from prolonged sitting, maintaining a healthy weight, and stopping smoking. None of these is a guaranteed cure, but together they support a healthier spine over the long run.
Why a second read can help
Disc findings are graded on a spectrum, and the same MRI can be described in noticeably different language depending on who reads it — a "bulge" to one radiologist may be a "small protrusion" to another, and the wording can shape whether surgery even enters the conversation. An expert second read of your spine MRI, which you can share with your own doctor, can confirm whether the finding truly explains your symptoms and how concerning it really is. Services like DocOrbit make it straightforward to get that independent review, and it is the same reasoning behind knowing when to get a second radiological opinion.
Does a herniated disc always need surgery?
No. The large majority of herniated discs improve with non-surgical care over weeks to a few months. Surgery is usually reserved for severe or worsening nerve compression, or pain that does not respond to conservative treatment. Your own doctor weighs your symptoms, exam, and MRI together before recommending it.
Can a herniated disc heal on its own?
Yes, this is common. Many herniations shrink over time as the body gradually reabsorbs the displaced disc material, and symptoms often ease even before the MRI changes. Most people feel substantially better within six to twelve weeks with conservative care.
What is the difference between a bulging disc and a herniated disc?
A bulging disc means the disc extends outward broadly but the outer wall is still intact, and it is often a normal age-related change. A herniation means inner disc material has pushed through a tear in the outer wall. Herniations are more likely to press on a nerve, but many cause no symptoms at all.
Is it safe to exercise with a herniated disc?
For most people, staying gently active is better than bed rest. Walking, swimming, and guided physical therapy usually help recovery. Avoid heavy lifting and sudden twisting during a flare, and check with your doctor or physiotherapist before starting a new program if you have leg weakness or numbness.
When should I worry about a herniated disc?
Seek prompt medical attention if you develop progressive leg weakness, numbness in the groin or inner thighs, or new loss of bladder or bowel control. These can signal serious nerve compression that needs urgent evaluation. For ordinary back or leg pain without these red flags, routine follow-up is usually enough.
Key takeaways
- A herniated disc is when soft inner disc material pushes through the disc's outer wall; it is very common and often painless.
- The MRI finding only matters when it lines up with your symptoms — incidental herniations are frequent.
- Most cases improve within weeks to a few months with activity, physical therapy, and pain relief, not surgery.
- Progressive weakness, groin numbness, or loss of bladder or bowel control are red flags that need urgent care.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.