If your brain MRI mentions "demyelinating plaques" or "demyelinating lesions," the words can be startling. That reaction is understandable, since they are so often linked in people's minds with multiple sclerosis. The reality is more nuanced. These patches in the brain's white matter have several possible causes, and the right next step depends on your symptoms, your history, and the look of the lesions themselves. This guide explains what radiologists mean by a demyelinating plaque, what conditions can produce them, when they matter most, and what evaluation usually looks like.
What "demyelinating plaques" means
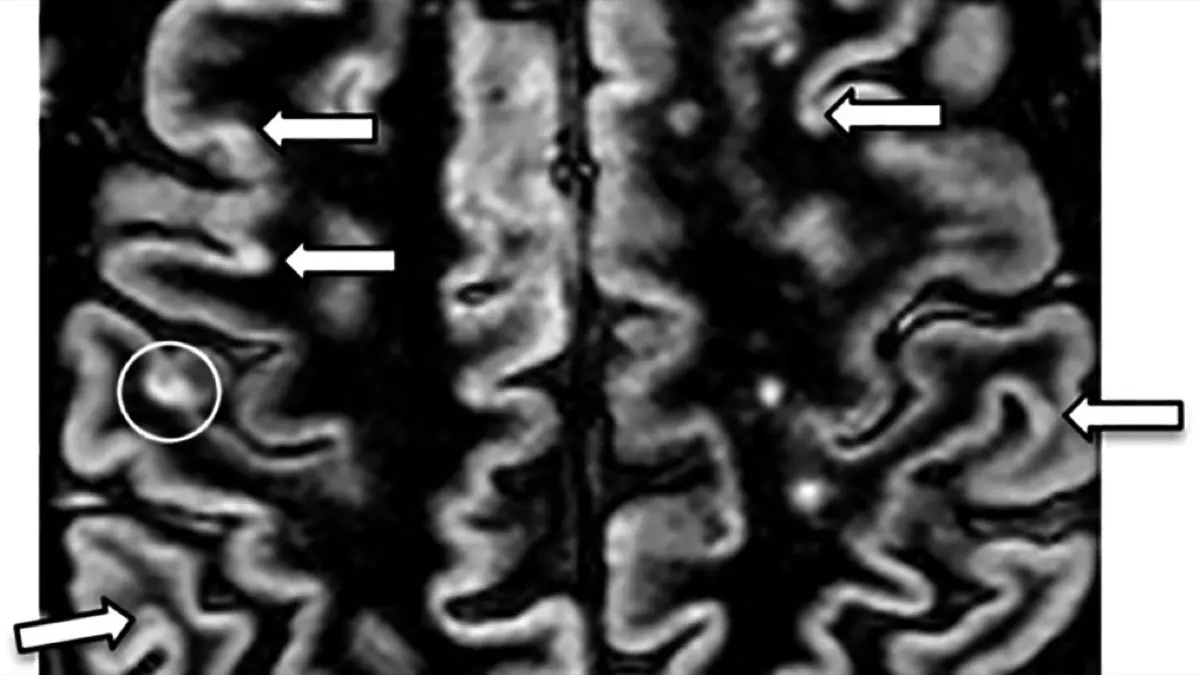
A demyelinating plaque is an area where myelin has been damaged. Myelin is the fatty insulation that wraps the nerve fibers in your brain and spinal cord. When myelin is injured, the nerves underneath cannot transmit signals as efficiently, and on MRI the affected patch shows up as a bright spot on FLAIR and T2-weighted sequences. Radiologists call these patches "plaques" or "lesions"; the words are used interchangeably in most reports.
Demyelinating plaques have characteristic features radiologists look for:
- Location: white matter, often around the ventricles (periventricular), in the corpus callosum, brainstem, cerebellum, or spinal cord.
- Shape: often oval or finger-like, sometimes oriented perpendicular to the ventricles (a pattern called "Dawson's fingers").
- Behavior on contrast: some lesions take up gadolinium contrast, which suggests recent or active injury. Others stay quiet, consistent with older damage.
Reports may also use phrases like "demyelinating lesions", "MS-like plaques", "ovoid white matter lesions", or "lesions suggestive of a demyelinating process".
Common causes
Multiple sclerosis (MS) is the best-known cause of demyelinating plaques, but it is not the only one. Other possibilities include:
- Clinically isolated syndrome (CIS): a single demyelinating event that may or may not evolve into MS over time.
- Neuromyelitis optica spectrum disorder (NMOSD): a distinct antibody-mediated condition that often involves the optic nerve and spinal cord.
- MOG antibody-associated disease: another antibody-driven cause, frequently with a different lesion pattern from MS.
- Acute disseminated encephalomyelitis (ADEM): most often after a viral infection, and more common in children.
- Post-infectious or post-vaccination demyelination: rare, and usually self-limited.
- Migraine-related white-matter foci: these can mimic plaques, but they usually do not enhance and tend to follow a different pattern.
It is also important to distinguish demyelinating plaques from chronic ischemic changes caused by small vessel disease. The two can look superficially similar on a single image, but the location, shape, and clinical setting usually point one way or the other.
Is it serious?
The honest answer is "it depends, and the workup is what tells you." A single, small, non-enhancing lesion in a person with no symptoms is a very different finding from multiple plaques distributed across typical MS locations with active enhancement. The distinction matters because:
- Active disease often benefits from early treatment. By active, we mean lesions that enhance with contrast or new lesions that appear over time.
- Old, stable plaques with no new ones over years usually mean the underlying process is quiet or well managed.
- Lesions that look like plaques but are not actually demyelinating do not need MS-specific treatment, and treating them as if they were would expose someone to unnecessary medication.
That is why the most important steps after an MRI showing demyelinating plaques are a careful neurological evaluation and, in many cases, a follow-up MRI to look for change over time.
Symptoms
Many demyelinating plaques are silent on the day they appear. When they do produce symptoms, the symptoms reflect the location of the plaque and often include:
- Numbness or tingling in a limb, the trunk, or the face.
- Weakness or clumsiness on one side of the body.
- Vision changes in one eye: pain with eye movement, along with blurred or dimmed vision, can suggest optic neuritis.
- Double vision.
- Imbalance, vertigo, or trouble walking.
- Bladder urgency, frequency, or hesitation.
- Fatigue.
Symptoms that come on over hours to days, last more than 24 hours, and then partially or fully resolve are particularly characteristic of demyelinating disease. Only a neurologist can put the picture together with the imaging and decide what the episode means.
How it is diagnosed and followed up
MRI is the cornerstone of the workup, but it is not the only piece. A typical evaluation includes:
- Brain MRI with contrast, often paired with cervical and thoracic spine MRI, because spinal-cord plaques carry diagnostic weight.
- Neurological examination by a neurologist or MS specialist.
- Bloodwork to rule out mimics: vitamin B12, thyroid, Lyme, syphilis, vasculitis markers, and antibodies such as aquaporin-4 (NMOSD) and MOG.
- Lumbar puncture (spinal tap) to look for oligoclonal bands, a finding often present in MS.
- Visual evoked potentials in selected cases to detect subclinical optic nerve involvement.
The diagnostic framework for MS, the McDonald criteria, requires evidence of damage in more than one part of the central nervous system and at more than one point in time. Sometimes those criteria are met on a single scan; sometimes they are met only after a follow-up MRI in 3–12 months. Patience with the diagnostic process is the rule rather than the exception.
Treatment options
Treatment depends on the specific cause and on how active the disease appears to be. The main approaches include:
- Disease-modifying therapies (DMTs) for MS. There are now many options, ranging from oral medications to infused therapies, chosen based on disease activity, side-effect profile, and patient preference.
- High-dose corticosteroids for an active relapse, to shorten its duration.
- Specific therapies for NMOSD or MOG disease, which differ from MS treatments and are guided by a specialist.
- Symptomatic treatments for spasticity, fatigue, pain, bladder problems, and mood.
Decisions about long-term treatment are made by a neurologist who can weigh imaging, exam, labs, and symptoms together. Starting the right treatment when it is genuinely indicated has a meaningful long-term effect; treating mimics carries its own risks.
Lifestyle changes
Lifestyle measures do not replace medical treatment, but they support brain health and may modify disease course in MS:
- Regular exercise: both aerobic activity and strength training.
- A balanced, anti-inflammatory style of eating, often a Mediterranean pattern.
- Adequate vitamin D, with levels checked by your doctor.
- Stopping smoking: smoking is consistently linked with worse MS outcomes.
- Good sleep, stress management, and treatment of co-existing conditions like high blood pressure and diabetes.
Why a second read can help
Demyelinating plaques sit in some of the more subjective territory of neuroradiology. Telling a true demyelinating pattern apart from small vessel disease, migraine-related white-matter foci, or other mimics takes careful interpretation, and so does judging activity from contrast behavior. A second read can confirm the lesion pattern is truly demyelinating, count and locate plaques accurately, and assess for activity. DocOrbit provides an expert second-opinion radiology report you can share with your neurologist. It can help before you start a long-term therapy, or when you want a clearer view of whether a neurological diagnosis is on solid ground.
Do demyelinating plaques always mean multiple sclerosis?
No. Multiple sclerosis is the most common cause of demyelinating plaques in adults, but several other conditions produce similar lesions, including NMOSD, MOG antibody disease, ADEM, and certain post-infectious processes. The pattern of lesions, your symptoms, and additional tests like blood antibodies and spinal fluid analysis are what point to one diagnosis over another. A neurologist puts these pieces together rather than relying on imaging alone.
Can demyelinating plaques disappear?
Some can shrink or look fainter on follow-up MRI, especially when they are recent and treated, but many leave a permanent mark on the scan even when the person feels fully recovered. What matters more clinically is whether new plaques are appearing, whether existing ones are enhancing, and whether the person has new symptoms. Stable imaging over time is one of the meaningful signs of good disease control.
How are demyelinating plaques diagnosed?
Diagnosis combines MRI of the brain and often the spinal cord with a neurological exam, blood tests, and frequently a lumbar puncture. The radiologist describes the lesions; the neurologist integrates those findings with your symptoms, exam, and labs to reach a specific diagnosis. Sometimes a single scan is enough; often a follow-up MRI in several months helps distinguish an isolated event from a chronic process.
Are demyelinating plaques the same as white-matter hyperintensities?
Not always. A white-matter hyperintensity simply describes a bright spot in the white matter on certain MRI sequences, and it can be caused by demyelination, small vessel disease, migraines, infections, or other processes. A demyelinating plaque is a specific type of white-matter hyperintensity with characteristic features: a periventricular location, an oval shape, and sometimes contrast enhancement. The radiologist tells one from the other based on those features and the clinical context.
Key takeaways
- Demyelinating plaques are areas of damage to nerve insulation, visible as bright spots on MRI in the brain's white matter and spinal cord.
- MS is one common cause among several. Others include NMOSD, MOG disease, ADEM, and post-infectious demyelination, plus mimics like small vessel disease.
- Diagnosis combines MRI, neurological exam, blood work, and often a lumbar puncture; a follow-up MRI is sometimes what clarifies the picture.
- Early, targeted treatment can meaningfully change long-term outcomes when the diagnosis is right. That is exactly why reaching the diagnosis with confidence matters so much.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.