If your MRI report mentions "chronic ischemic changes," it is one of the most common phrases a brain MRI ever produces — and for the large majority of people, it is not the alarming finding it sounds like. It usually describes long-standing wear on the brain's small blood vessels, the kind that accumulates quietly with age and vascular risk factors. This guide explains what radiologists actually mean by the term, what causes it, when it matters clinically, and what the typical follow-up looks like.
What chronic ischemic changes actually mean
"Ischemia" simply means reduced blood flow. "Chronic ischemic changes" therefore describes the lasting marks left in brain tissue by years of slightly reduced blood supply through the smallest blood vessels of the brain. These vessels feed the deep white matter — the cabling that connects different parts of the brain — and they are particularly sensitive to high blood pressure, diabetes, and aging.
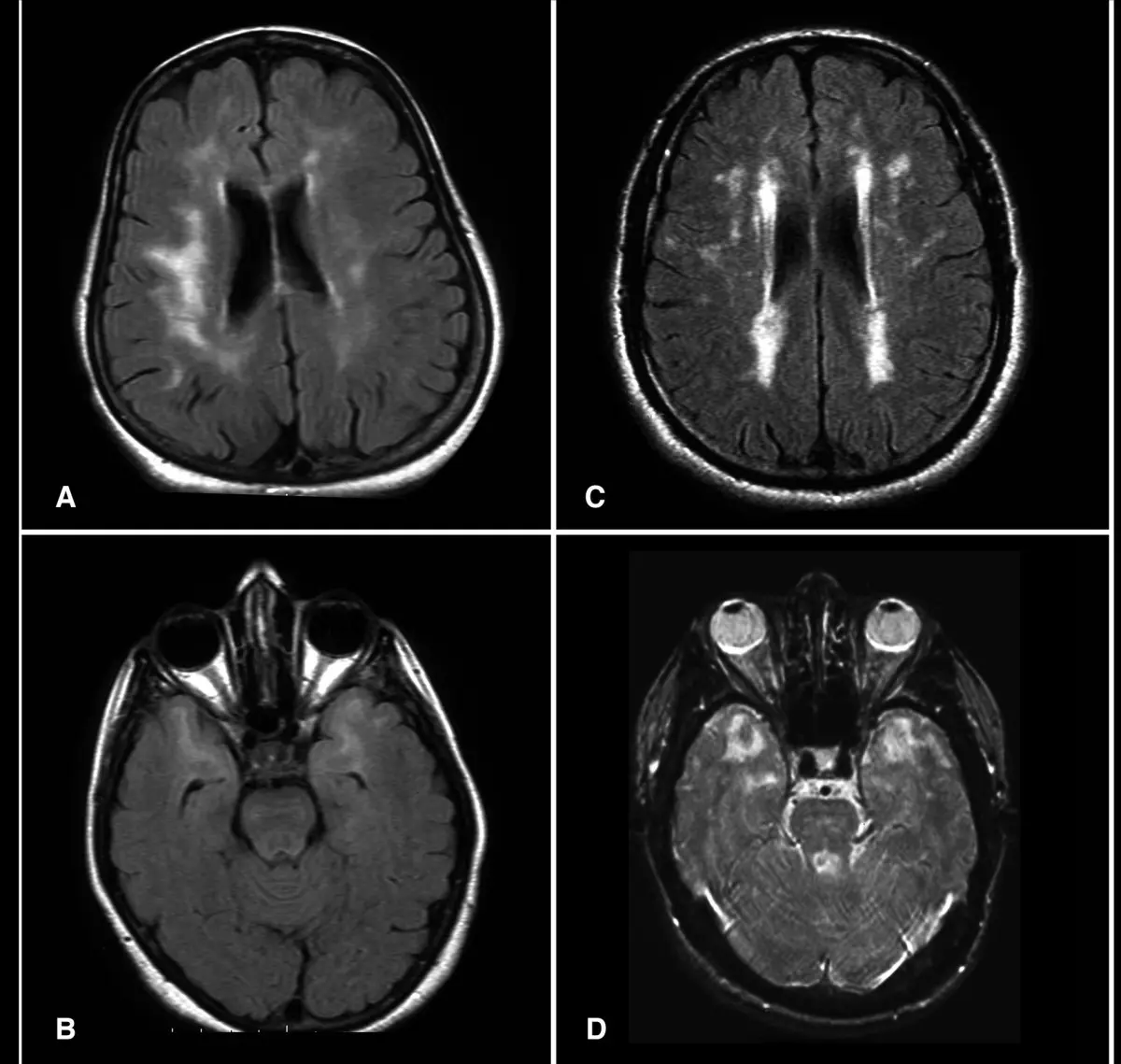
On an MRI these changes appear as small bright spots or patchy areas, mainly on the FLAIR and T2 sequences. Radiologists describe them in different ways depending on how much white matter is involved:
- Punctate or focal white-matter hyperintensities — a few small dots, often in older adults.
- Confluent white-matter changes — larger patches where several small areas have merged together.
- Periventricular and deep white-matter changes — describing where in the brain the changes appear.
You may also see the terms "small-vessel ischemic disease," "leukoaraiosis," or "white-matter hyperintensities of presumed vascular origin." For practical purposes these all describe the same family of findings.
What causes them
Chronic ischemic changes are not caused by a single event. They build up over time from the same risk factors that drive heart and vascular disease:
- High blood pressure — the single biggest contributor, especially when long-standing or poorly controlled.
- Diabetes and insulin resistance — damage small vessels throughout the body, including the brain.
- High cholesterol and atherosclerosis — narrow and stiffen the vessels that feed the brain.
- Smoking — accelerates small-vessel damage.
- Older age — some white-matter change is common even in healthy older adults.
- Sleep apnea — repeated drops in oxygen at night can stress brain tissue.
Because the same risk factors damage the heart's arteries, doctors often think of chronic ischemic changes as a quiet signal that vascular health deserves attention — even when the brain itself feels fine.
Are they serious?
For most patients, especially over 50, a small amount of chronic ischemic change on MRI is an age-related finding rather than a disease. What matters is the overall picture:
- Mild, stable changes in an older adult with controlled vascular risk factors are common and usually not actionable on their own.
- Moderate to severe changes, especially if they appear "out of proportion" for the patient's age, are taken more seriously. They are associated with a higher risk of stroke, gait problems, and cognitive decline if vascular risk factors are not addressed.
- Rapidly progressing changes on repeat imaging, or changes combined with small old infarcts or microbleeds, warrant a closer neurological look.
Severity is not something to estimate from the report alone. A neurologist or a careful second read on the images themselves is the right way to put a number on it — and to compare with any older scans you have.
Symptoms — and the very common case of no symptoms
Most people with mild chronic ischemic changes have no symptoms at all. The findings are picked up incidentally when an MRI is ordered for an unrelated reason — headaches, dizziness, or a head injury. When the changes are more extensive, however, possible symptoms include:
- Slower thinking, mild memory or attention problems.
- Mood changes, including new low mood or apathy.
- Subtle gait or balance issues, especially in older adults.
- Increased risk of falls.
None of these symptoms is specific to chronic ischemic changes — many other conditions can cause them. That is exactly why the radiology report is the start of the conversation with your doctor, not the answer.
How they're followed up
There is no single rule for follow-up. The plan depends on how extensive the changes are, your age, your vascular risk profile, and whether you have neurological symptoms. In practice, doctors usually do some combination of:
- Optimizing risk factors first. Blood pressure, blood sugar, cholesterol, and smoking are all treatable.
- A neurology or stroke clinic referral if the burden is moderate to severe, or if symptoms are present.
- A repeat MRI after one to two years in selected cases, to see whether changes are stable or progressing.
- Cognitive screening if memory or thinking symptoms are reported.
Follow-up recommendations vary by patient. Your own doctor knows your history, your symptoms, and any earlier scans — together those usually settle the right cadence.
Treatment and lifestyle changes
There is no medication that erases existing chronic ischemic changes. The whole strategy is to slow the appearance of new ones and to protect against stroke. The evidence-backed levers are familiar:
- Treat high blood pressure to target — this is the single most impactful step.
- Keep diabetes well controlled.
- Manage cholesterol, often with a statin if your overall cardiovascular risk is elevated.
- Stop smoking. Even years-long smokers see benefit from quitting.
- Aim for regular aerobic activity — most weeks, most days.
- Address sleep apnea if it is present.
- Discuss antiplatelet therapy (such as aspirin) only with your doctor — it is not appropriate for everyone.
These steps protect the heart, the brain, and the rest of the vascular system at the same time. Even modest improvements compound over the years.
Why a second read can help
"Chronic ischemic changes" covers a wide spectrum, from a couple of small dots to extensive confluent disease. The clinical implications are very different at each end, and that grading can be subjective. A focused second read of your MRI — comparing your current scan with any prior imaging, and grading the burden on the standard Fazekas scale — can sharpen the picture and give you something concrete to discuss with your neurologist. DocOrbit's expert second-opinion service is built for exactly this kind of question: you upload the scan, a subspecialist reviews it, and you get a clear written report you can share with your own doctor. If a neurological finding leaves you unsure, our note on when a second neurological opinion can make a difference is a good place to start. You can also read when to get a second radiological opinion in general.
Are chronic ischemic changes the same as a stroke?
No. Chronic ischemic changes describe long-standing wear on the brain's small blood vessels, while a stroke is a sudden, focal loss of blood flow that damages a specific area. The two can coexist, but seeing chronic ischemic changes on an MRI does not mean a stroke happened. A radiologist will say so directly if a stroke is suspected.
Can chronic ischemic changes be reversed?
The existing white-matter changes themselves are not reversible, because they reflect tissue that has already adapted to long-term low blood flow. What you can change is the trajectory: treating blood pressure, diabetes, and cholesterol, stopping smoking, and staying physically active have all been shown to slow how fast new changes appear. Progression is the part that matters most.
Do chronic ischemic changes always cause dementia?
No. Many older adults have mild chronic ischemic changes on MRI and never develop noticeable cognitive problems. The risk goes up when the changes are extensive, progressing quickly, or combined with other findings — but a small, stable burden in an older patient is most often an age-related finding rather than a sign of impending dementia.
What lifestyle changes help slow chronic ischemic changes?
The biggest levers are controlling blood pressure, keeping blood sugar and cholesterol in target ranges, quitting smoking, sleeping well, and exercising regularly. These are the same vascular risk factors that drive heart disease, and managing them protects both the brain and the heart. Even modest improvements over years can change how much new damage accumulates.
Key takeaways
- Chronic ischemic changes are long-standing wear on the brain's small blood vessels — common with age and vascular risk factors, not a sudden event like a stroke.
- A small, stable burden in an older patient is usually incidental. Moderate to severe or progressing changes deserve closer attention.
- The most powerful response is treating the underlying risk factors — blood pressure first, then diabetes, cholesterol, smoking, and activity.
- If the report leaves you uncertain about severity, a focused second read can grade the changes and put them in clinical context.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.