If your MRI report mentions "cerebral atrophy," the word sounds dramatic, but in the large majority of cases it is a description rather than a diagnosis. It usually means the brain looks slightly smaller than the typical reference for your age — most often because of normal aging, sometimes because of a specific condition that needs attention. This guide explains what cerebral atrophy actually is, what causes it, how doctors decide whether it matters, and what the usual next steps look like.
What cerebral atrophy actually means
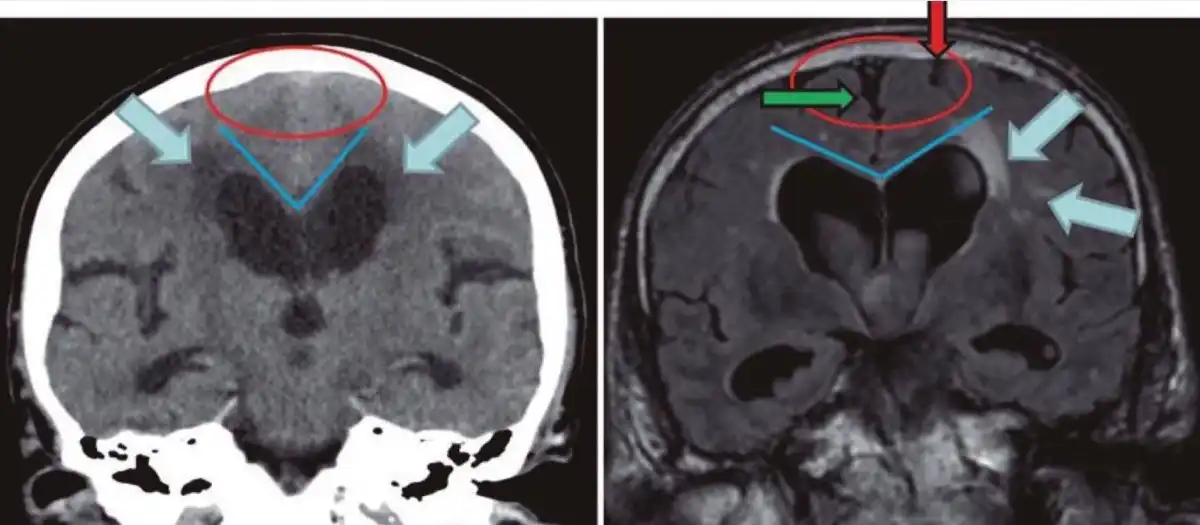
Cerebral atrophy is the loss of brain tissue volume. Radiologists do not weigh your brain; they look at landmarks. On an MRI, two patterns commonly suggest atrophy:
- The folds on the surface of the brain (called sulci) look wider than expected.
- The fluid-filled spaces inside the brain (called ventricles) look larger than expected.
When the brain shrinks slightly, the surrounding cerebrospinal fluid fills the extra room. That is why atrophy is often described together with phrases like "prominent CSF spaces," "ex vacuo dilatation of the ventricles," or "sulcal widening."
Radiologists also try to compare what they see to what is typical for your age. The report may use phrases like:
- Mild generalized cerebral atrophy — modest, evenly distributed volume loss.
- Atrophy appropriate for age — the change is within the expected range for someone your age.
- Atrophy more than expected for age — the brain looks older than the patient.
- Focal atrophy — one region (frontal lobes, temporal lobes, hippocampus, cerebellum) is more affected than the rest.
The location and the degree relative to your age are the two pieces of information that matter most clinically.
What causes cerebral atrophy
Cerebral atrophy is not a single condition; it is a common endpoint of several different processes. The most frequent contributors include:
- Aging — the brain naturally loses a small fraction of its volume each decade after about age 30. Most older adults show some sulcal widening on MRI without any cognitive symptoms.
- High blood pressure, diabetes, and small-vessel disease — long-standing vascular damage can accelerate brain volume loss. This often shows up alongside chronic ischemic changes on the same MRI.
- Alzheimer's disease and other neurodegenerative conditions — these tend to cause focal patterns, especially atrophy of the hippocampus and medial temporal lobes early on.
- Frontotemporal dementia — disproportionate atrophy of the frontal and anterior temporal lobes.
- Parkinson's disease and atypical parkinsonian syndromes — can produce midbrain or cerebellar atrophy.
- Chronic heavy alcohol use — can cause both global atrophy and a specific pattern of cerebellar volume loss.
- Past brain injury — head trauma, stroke, infection, or radiation therapy can leave focal atrophy in the regions they affected.
- Multiple sclerosis and other inflammatory conditions — can drive brain volume loss over time.
- Severe long-standing illness, sleep apnea, malnutrition — chronic low-grade stress on brain tissue.
Many people have more than one of these factors at play. The radiologist is not always able to tell which cause is dominant from the MRI alone — that is a job for the clinician who knows your history.
When cerebral atrophy is age-related and when it is concerning
Some volume loss with age is normal — comparable to the way a 70-year-old's heart, lungs, or skin look different from a 20-year-old's. What concerns doctors is not the presence of atrophy but the pattern:
- Age-related (common, usually reassuring) — mild, evenly distributed atrophy in someone over 60, no significant cognitive complaints, no focal pattern.
- More than expected for age — the same pattern but in a younger patient, or noticeably advanced in an older one.
- Focal atrophy — disproportionate volume loss in a specific region (hippocampal, frontal, cerebellar) usually triggers a closer look.
- Rapid progression — when atrophy is clearly worse on a follow-up MRI compared with one taken a year or two earlier.
The same MRI report can be reassuring in one patient and a flag in another. A 78-year-old with mild generalized atrophy and a sharp memory is in a very different situation than a 55-year-old with the same finding and new memory complaints.
Symptoms
Most people with mild, age-related cerebral atrophy have no symptoms at all. When symptoms do occur, they reflect the area of the brain that has lost volume:
- Memory difficulty and word-finding trouble — often associated with hippocampal and temporal-lobe atrophy.
- Personality, judgment, or behavior change — can accompany frontal-lobe atrophy.
- Coordination, balance, or gait problems — may follow cerebellar volume loss.
- Slowed thinking, attention, and multitasking trouble — common when diffuse atrophy and small-vessel disease occur together.
Symptoms — not the MRI report alone — drive whether further evaluation is needed.
How cerebral atrophy is followed up
There is no fixed schedule. The next steps depend on the pattern of atrophy, the patient's symptoms, and the clinician's overall impression:
- Mild atrophy, no symptoms — usually no follow-up imaging beyond what is already planned for other reasons. The radiologist may simply note it for the record.
- Cognitive symptoms — typically a referral to a neurologist or memory clinic for formal cognitive testing, blood work (thyroid, B12, glucose, sometimes infectious testing), and sometimes a repeat MRI in 6–12 months to assess progression.
- Focal or unexpected pattern — may prompt additional studies: a dedicated dementia MRI protocol, FDG-PET, amyloid PET, or cerebrospinal fluid analysis in selected patients.
- Specific differential concerns — the workup is tailored to the suspected condition (vascular, neurodegenerative, alcohol-related, inflammatory).
The radiology report describes the structure; your neurologist or primary care doctor adds the clinical picture.
Treatment and lifestyle
There is no medication that reverses cerebral atrophy. The realistic goals are to treat any underlying condition that is driving it and to slow the rate at which new changes accumulate. The same vascular risk factors that drive heart disease also affect the brain:
- Blood pressure control — the single largest lever for brain volume loss tied to vascular causes.
- Diabetes and cholesterol management — keep these in target ranges.
- Stop smoking — accelerates small-vessel damage.
- Regular aerobic exercise — repeatedly linked to better preserved brain volume in long-term studies.
- Sleep, including treatment of sleep apnea if present — chronic low oxygen at night is harder on the brain than most people realize.
- Treat depression, hearing loss, and social isolation — modifiable risk factors that show up in dementia prevention studies.
- Limit heavy alcohol — particularly relevant when alcohol-related atrophy is in the differential.
When a specific neurodegenerative disease is identified, treatments are condition-specific (for example, cholinesterase inhibitors or anti-amyloid therapies in selected Alzheimer's patients). These do not regrow brain tissue, but they can affect day-to-day function.
Why a second read can help
Two readers can interpret the same MRI very differently — especially when the central question is "how much atrophy is appropriate for this age?" A second neuroradiology read can pick up subtle focal patterns, confirm or moderate the original impression, and give your treating doctor a clearer baseline to follow over time. DocOrbit provides an expert second-opinion radiology report you can share with your own physician — useful when the first report uses ambiguous language or when the next step would mean starting a workup that depends heavily on how the MRI is interpreted. For neurological findings specifically, it can also help to read why a second opinion in neurology matters.
Is cerebral atrophy the same as dementia?
No. Cerebral atrophy is an imaging finding — visible loss of brain volume on a scan. Dementia is a clinical syndrome of cognitive decline that interferes with daily life. The two can be related, especially in Alzheimer's disease, but many people have mild atrophy on MRI and normal cognition, and dementia can be diagnosed before clear atrophy appears. The diagnosis depends on clinical assessment, not the MRI report alone.
Can cerebral atrophy be reversed?
Lost brain tissue does not grow back, so the existing atrophy cannot be reversed. What can change is the trajectory: treating vascular risk factors, exercising regularly, sleeping well, and addressing any specific underlying disease have all been associated with slower future volume loss. Progression is the part that responds to action.
Is mild cerebral atrophy normal at my age?
Some cerebral atrophy is expected with age — the brain naturally loses a small percentage of its volume each decade after the 30s. In older adults, mild generalized atrophy on MRI in the absence of cognitive symptoms is usually considered age-appropriate. What matters is whether the degree is out of proportion to your age and whether the pattern is focal or diffuse.
Does cerebral atrophy mean I will develop Alzheimer's?
Not on its own. Alzheimer's disease is associated with specific patterns of atrophy, especially in the hippocampus and medial temporal lobes, but generalized mild atrophy in an older adult does not predict it. The MRI is one piece of a clinical picture that also includes memory testing, history, and sometimes additional tests. Your neurologist or primary care doctor is in the best position to put those pieces together.
Key takeaways
- Cerebral atrophy on MRI describes brain volume loss, usually visible as widened sulci and slightly larger ventricles.
- Some atrophy is expected with age; the pattern and degree relative to your age matter most.
- Vascular risk factors drive much of the preventable atrophy — controlling blood pressure, diabetes, and lifestyle factors helps slow progression.
- The MRI is not a diagnosis on its own; clinical correlation with symptoms and history is what decides next steps.
- A second neuroradiology read can clarify ambiguous or borderline reports.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.