Few phrases on a scan report send people straight to the search bar like "atherosclerotic plaque." If you have just read those words on a carotid ultrasound, a CT of your chest, or a report on the arteries in your neck, abdomen, or legs, here is the reassuring starting point: plaque in the arteries is extremely common as we age, it builds up slowly over many years, and finding it is often genuinely useful news, because almost everything that drives it can be measured and managed.
What does "atherosclerotic plaque" mean?
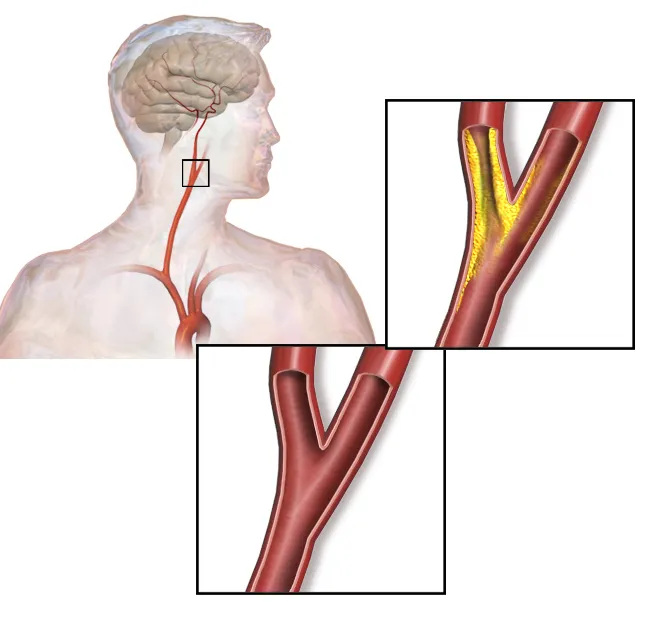
Plaque is a buildup of cholesterol, fat, calcium, and other cells inside the wall of an artery. The process that creates it is called atherosclerosis, sometimes written as "atheromatous" or "atheromatous changes" on a report. Over time these deposits can thicken the artery wall and, in some places, narrow the channel that blood flows through.
Radiologists pick it up on several kinds of imaging, and the wording depends on where it is seen:
- Carotid ultrasound (neck arteries), wall thickening and plaque, often with a measured percentage of narrowing
- CT, calcified plaque shows up bright white; a "coronary calcium score" estimates buildup in the heart's arteries
- MRI and CT/MR angiography, map the artery and any narrowing in detail
- Doppler ultrasound of the legs, checks flow in the limb arteries
You will often see plaque described as calcified (hardened, more stable), non-calcified or "soft" (fattier, slightly more prone to rupture), or mixed. The other key number is the degree of stenosis, how much the artery is narrowed.
Common causes and risk factors
Atherosclerosis develops from a combination of factors acting over years, not from any single cause. The most common contributors are:
- Rising age, some buildup is almost universal in older adults
- High LDL ("bad") cholesterol
- High blood pressure
- Smoking
- Diabetes or high blood sugar
- Family history of early heart disease or stroke
- Excess weight, low physical activity, and a diet high in processed and saturated fats
The encouraging part is that most of these are modifiable. Plaque is partly a record of your past risk, but the future trajectory is something you and your doctor can influence.
Is it serious?
It depends on three things: where the plaque is, how much it narrows the artery, and whether it is causing symptoms. A small amount of incidental, calcified plaque noted on a scan done for another reason is common and usually managed with risk-factor control rather than alarm. Significant narrowing in a carotid or coronary artery is a different conversation, that is the kind of finding doctors take seriously and act on in a planned way.
Plaque matters because of what it can lead to: a narrowed artery limits blood flow, and an unstable plaque can rupture and trigger a clot. In the brain's circulation, the downstream effects can resemble the small-vessel findings discussed in our articles on chronic ischemic changes and lacunar infarcts. Seeing plaque early is precisely what gives you and your doctor the chance to lower that risk before it causes a problem.
What symptoms can it cause?
For years, often none. Plaque builds quietly, which is exactly why it is so often found incidentally. When symptoms do appear, they reflect the artery involved: chest pain or breathlessness on exertion with the heart's arteries; brief weakness, numbness, slurred speech, or vision changes (warning signs of a transient ischemic attack) with the carotids; and leg cramping or pain when walking that eases with rest with the leg arteries. Any sudden neurological symptoms should be treated as an emergency.
How is it diagnosed and followed up?
A report mentioning plaque is usually the start of a picture, not the whole story. Depending on the location and amount, your doctor may add a lipid panel and blood pressure review, a carotid ultrasound follow-up at intervals, a coronary calcium score or stress test for the heart, or, when narrowing looks significant, a CT or MR angiogram. Imaging is always read alongside your symptoms, history, and bloodwork; the same scan finding can mean different things in different people.
Treatment options
For most people, "treatment" means managing risk rather than a procedure. Doctors commonly use statins to lower cholesterol and stabilize plaque, medications to control blood pressure and diabetes, and sometimes a low-dose antiplatelet such as aspirin when the overall risk justifies it. Procedures like carotid surgery (endarterectomy), stenting, or bypass are reserved for significant narrowing or symptoms, and those decisions are individualized. The aim is not to erase every speck of calcium but to keep plaque stable and blood flowing.
Lifestyle changes that genuinely help
This is one area where day-to-day choices clearly move the needle. Stopping smoking is the single highest-impact change. Regular physical activity, a diet leaning toward vegetables, whole grains, fish, and healthy fats, keeping weight and blood sugar in a healthy range, and treating high blood pressure all slow the process and help stabilize existing plaque. None of this has to happen overnight, steady, sustainable changes matter more than dramatic ones.
Why a second read can help
The degree of narrowing, the type of plaque, and whether a borderline measurement crosses a treatment threshold are all judgement calls that can vary between readers, and they can change what gets recommended next. An expert second read, like the one DocOrbit provides, gives you a clear, independent interpretation of your imaging that you can bring to your own doctor. If you are weighing whether it is worth it, our guide on when to get a second radiological opinion walks through the situations where it adds the most value.
Is atherosclerotic plaque dangerous?
By itself, finding some plaque is very common with age and is not an emergency. What matters is where it is, how much it narrows the artery, and whether it is causing symptoms. Mild, calcified plaque is usually managed with risk-factor control, while significant narrowing in a carotid or coronary artery is something doctors monitor and treat more actively.
Can atherosclerotic plaque be reversed?
Established plaque rarely disappears completely, but the process can often be slowed, stabilized, and partly improved. With statins, blood-pressure control, not smoking, and an active lifestyle, plaques can become more stable and less likely to cause problems, even if the calcium they contain stays visible on scans.
What is the difference between calcified and soft plaque?
Calcified plaque is older, hardened buildup that shows up bright on CT and tends to be more stable. Soft (non-calcified) plaque is fattier and is statistically more prone to rupture, which is what can trigger a clot. Many plaques are mixed. Your doctor weighs plaque type alongside how much the artery is narrowed.
Does atherosclerotic plaque always need treatment?
Not always in the sense of a procedure, but it is almost always a signal to manage your cardiovascular risk. For most people that means lifestyle changes and sometimes medication. Procedures like stenting or surgery are reserved for significant narrowing or symptoms, and that decision depends on your full clinical picture.
What causes plaque to build up in arteries?
Plaque builds up over years from a mix of high LDL cholesterol, high blood pressure, smoking, diabetes, age, and genetics. The artery wall reacts to injury and cholesterol by laying down fatty deposits that gradually harden. Most of these drivers can be measured and, importantly, improved.
Key takeaways
- Atherosclerotic plaque is a very common buildup of cholesterol, fat, and calcium in artery walls, and finding it is often a useful early warning rather than an emergency.
- What matters most is the location, the degree of narrowing, plaque type, and whether you have symptoms.
- Most of the drivers, cholesterol, blood pressure, smoking, diabetes, are measurable and improvable.
- Treatment ranges from lifestyle changes and medication to procedures only when narrowing or symptoms are significant.
- Interpretation always depends on your symptoms, history, and labs, so discuss your specific report with your doctor.
This article is for general information only and is not medical advice. Always discuss your imaging results and any next steps with a qualified physician.